INTRODUCTIONTechnology development in Brazil, especially in big cities, has generated high rates of pollution, particularly noise pollution. Traffic noise is considered one of the worst noise pollution. It is mentioned in scientific publications as well as in popular media (newspapers, magazines and television). São Paulo city presents unfavorable acoustic features caused by intense population.
Noise-induced hearing loss can cause a quantity reduction of hearing ability as well as a quality change, as sound is distortedly noticed - called recruitment phenomenon. It makes dynamic area of hearing is reduced. Thus, the same individual who is not able to hear less intense stimulus may present an excessive sensitiveness to heavy sounds, and so perception of these stimulus become deformed and uncomfortable (Azevedo et al., 1993).
Alterations or even effects caused by noise to hearing and to health in general terms, are influenced by SPL, by type of sound, by frequency, by time exposure to noise and even by individual sensitiveness. In this way, noise can affect individuals in different manners exposed to the same period of time (Linden, 1996).
Marques (1998) pointed out that visual or haring disability on professional drivers can cause damages not only to their physical integrity but also to their passengers, and even to pedestrians. Disorders on health and on quality of life also influence professional performance. Besides hearing symptoms, a great amount of alterations can be determined by the excess of occupational noise, such as: cardiovascular disturbances as Systemic Artery Hypertension (Corrêa Filho et al., 2002; Souza and Silva, 2005), muscle skeletal alterations due to vibrations exposure (Balbinot and Tamagna, 2002; Silva and Mendes, 2005), digestive, behavior, nerological, vestibular disturbances, sleep and communication alterations. Neri, Soares and Soares (2005) pointed that the average missing days due to any health problems on (bus) drivers was 6.28 days, what showed a pay loss of about R$ 6.6 million in the stated of Ba, RJ, SP and MG.
Rossi (1999) researched audiological profile from ambulance drivers, who became potential candidates to obtaining health problems caused by sound pollution. He performed audiometry tests in 36 ambulance drives, aging from 33 to 62 years. 32 from those were male and four female. Results from audiometry showed that 58.33% of the individuals had some hearing alteration, and from those 76.19% presented audiometry curves suggesting noise-induced hearing loss.
According to Fiorini (2000), environmental impact can be one of the main consequences of technology and science advances which distinguish the end of the second millennium. The search for technology development represents not only the tendency to human progress, but also important changes on Quality of life of the individuals. In this way, despite the advantages from progress, environmental impact can also cause implications on health, therefore, they deserve especial attention from health professionals.
Sanches (2003) assigned that sources of urban noise are many. They can be from cars, buses, police and ambulance siren and even the ones related to pleasure. Noise causes important damages to physical and mental health, so population should be aware of it.
The most frequent complaints by individuals with hearing impairment are not related to hearing difficulty, but to speech understanding, which can bring serious consequences to their professional, social and family life. This type of complaint shows how much ability of hearing recognition is fundamental to social and emotional welfare of any individual. When classifying hearing only by figures from tonal audiometry, we can suppose difficult grade the subject will present, but we cannot assure such expectation. Hearing ability is not only quantity, but mainly, quality (Momensohn-Santos and Russo, 2005).
We verified that, in this revision of literature, there is a shortage of scientific studies on effects of noise on hearing of ambulance drivers. An audiological profile for this professional class has not been written yet. So, the hypotheses are:
1. It is expected that such professionals have hearing threshold according to standard of normality or sensorineural hearing loss in high, middle-high frequencies, which are features from noise-induced hearing loss.
2. If we find hearing loss, left ear will be the most affected for being the one which is closest to the ambulance car window and, though, is directly exposed to environmental sound.
TARGETThis work has aimed a descriptive study of audilogical profile from ambulance drivers, under audiometric and measures of acoustic impedance aspects. Urban noise, stressed by sirens, is an important exogenous factor when determining such profile, and it can cause a type of hearing loss which is typical from these physical agents on these drivers.
MATERIAL AND METHODThis study was done at Aprimoramento de "Saúde e Trabalho" do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo - HCFMUSP (Health and Labor Department at HCFMUSP)
We analyzed audiological tests from ambulance drivers from two great public hospitals, in São Paulo city: Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HCFMUSP) and Instituto de Infectologia Emílio Ribas (ER).
Characteristics and convocation of individualsWe studied 28 male, ambulance drivers. These patients were invited to take part of the research through an invitation letter provided after a doctor visit at Ambulatório de Otorrinolaringologia Ocupacional (Occupational ENT Ambulatory) - HCFMUSP, as well as at Serviço de Saúde Ocupacional do Instituto de Infectologia Emílio Ribas (Occupational Health Service of Institute of Infectiology). If drivers became interested, doctors would send them to appoint a visit at Serviço de Saúde Ocupacional - SSO-HCFMUSP, where research was done. The criteria of sample selection were:
- Working only as an ambulance driver.
- Two-year-experiences at least.
- Eight-hour-working day as average.
- Not over 63 years old.
- Absence of alteration on middle ear and conductive hearing loss.
- Absence of unilateral, sensorineural hearing loss, from severe to profound grades in all frequencies.
Ethics ConsiderationsThis study was presented and approved by Comissão de Pesquisa do Centro de Aprimoramento de Pessoal (CEAP) - Instituto Central do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (IC-HCFMUSP).
Free and Clear Consent TermAfter approval from drivers in taking part of the research, it was presented to them a free and clear consent term, which was read and signed before beginning the study. A copy of it was handed in to drivers and another was filed by the responsible doctor of the research. We made sure they would have assistance even if they did not take part in the research.
Procedures
AnamnesisThe subjects were submitted to an occupational and clinic anamnesis as well as a specific anamnesis to ambulance drivers.
Visual Inspection of the External Acoustic Meatus and Tonal Audiometry- Visual Inspection of the External Acoustic Meatus (verification of some impossibility to perform test such as partial or total cerumen on the external acoustic meatus). We made use of otoscope Heine mini 2000. If any alterations occurred, we would send patient to an ENT doctor from SSO-HCFMUSP or to Ambulatório de Otorrinolaringologia Ocupacional - HCFMUSP.
- Tone audiometry with 14-hour-hearing rest to be performed, in frequencies of 0.25 kHz, 0.5 kHz, 1 kHz, 2 kHz, 3 kHz, 4 kHz, 6 kHz through air passages and 8 kHz through bone passages. Speech audiometry with speech recognition threshold and speech recognition index. It was used audiometer Siemens, model SD 25, yearly calibrated according to the proposed criteria by Momensohn -Santos and Russo (2005).
- Accoustic impedance measures (tympanometry and threshold measures from estapedial, ipsilateral and contralateral reflexes), performed with impedanceometer AZ 7 Interacoustics, also yearly calibrated.
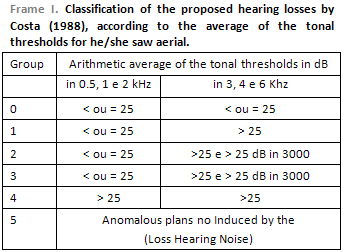
Criteria of result analysis We made use of the criteria proposed by Costa (1988) to classify audiometric threshold from ambulance drivers.
According to Frame 1, group 0, we found audiograms whose losses are under 25 dB in all frequencies or in their averages. In group 5, there are traces corresponding to non-occupational losses. Noise-induced hearing loss which presents falls between 3 and 6 kHz are classified in group from 1 to 4. Then, two arithmetic averages from hearing loss in dB occur. The first average, in 0.5, 1 and 2 kHz shows quality of hearing discrimination in acoustically designed booth. The second one, in 3, 4 and 6 kHz, characterizes noise-induced hearing loss. Implications in 3 kHz and then in 2 kHz shows development of lesions in terms of intelligibility in everyday conditions. In the classification of groups 3, 4 and 5, it is recommended that such workers should be sent to ENT evaluation. The two averages are important to quantify audiometric deviations which might occur year after year.
We also performed Objective Recruitment Research by Metz. The presence of recruitment occurs when the intensity difference between tonal threshold and threshold of estapedial reflex is reduced, i.e. lower than 60 dB. In individuals with normal hearing, this difference is from 70 to 90 dB (Momensohn-Santos and Russo, 2005).
Statiscal AnalysisStatistical tests were used (Student´s t-test, Mann-Whitney test, Wilcoxon signed-rank test and analysis of Spearman correlation) with level of significance of 5% (p<0.050), recommended to biological studies.
In the analysis of Spearman correlation, the positive sign meant that the greater the occurrence from the first variable studied, the greater the second will be. Therefore, the negative sign represented the opposite: the lower the variable studied, the greater the second will be.
RESULTSComparing the groups from Instituto de Infectologia Emílio Ribas (ER) and from Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HCFMUSP) (Student´s t-test), we observed that age was similar in the two groups (p = 0.126).
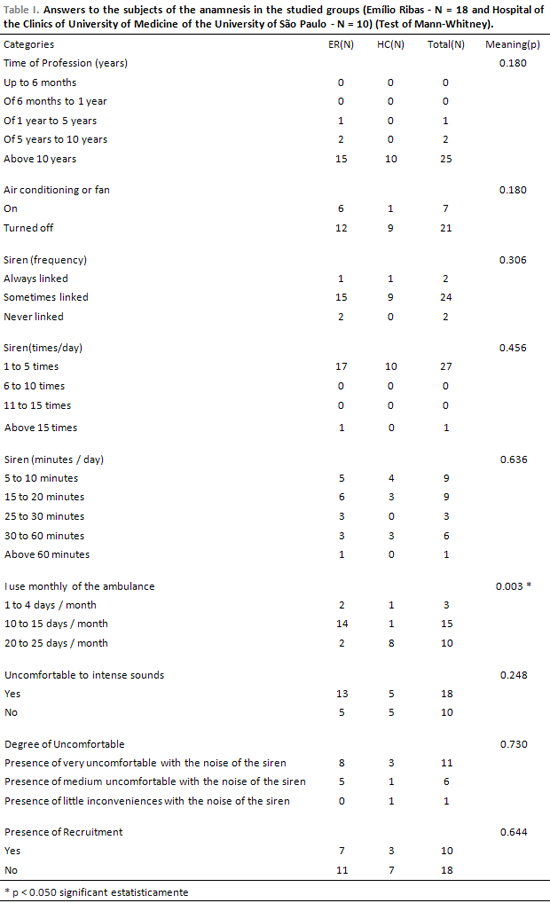
In Table 2, we observed that there was a significant statistical difference only to the category "monthly use of ambulance" between groups from Instituto de Infectologia Emílio Ribas and from Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, with p = 0.003, showing that drivers from the latter make more use of ambulance than drivers from the former. To the other categories, there was no significant statistical difference between responses from both hospitals´ drivers.
All individuals during anamnesis (n=28) reported leaving ambulance window opened when driving (100%).
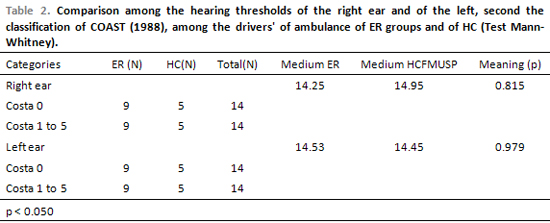
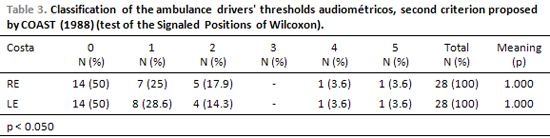
Through Mann-Whitney test, we observed that there was no significant statistical difference when compared with COSTA´s classification in right ear (RE) (p=0.815) and COSTA´s in left ear (LE) (p=0.979) between ER and HCFMUSP, this means that patients from both hospitals can be gathered in only one category - ambulance drivers (Table 2). Therefore, in Table 3, we noticed that there was no significant statistical difference (p=1.000) between classifications of hearing loss in the right ear with classification of hearing loss in the left ear when drivers´ ears from both hospitals were gathered.
DISCUSSIONTraffic noise is one of the greatest causes of increasing of sound pressure levels (SPL) in big cities. Many people relate noise to progress, consumism, habits, fashion and amusement (Marques, 1998; Fiorini, 2000). Nevertheless, it can cause an uncomfortable subjective sensation to individuals, especially when in unexpected and intense levels. These different effects caused by noise to man, organic, psychological as well as social, have been studied by several professionals in the area, including phonoaudiology.
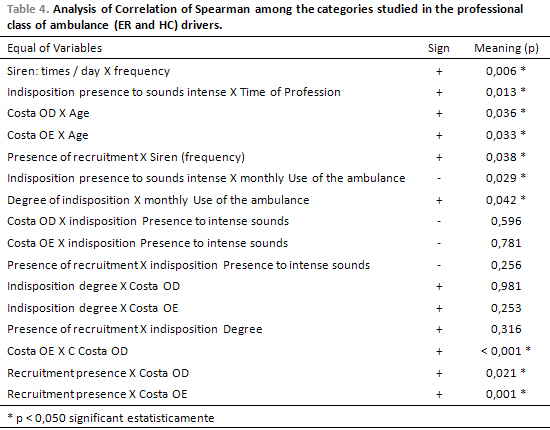
In Table 1, in relation to anamnesis response, we noticed a subjective aspect mainly in questions related to the frequency the ambulance siren was on (always, sometimes or never) and when its noise caused discomfort (a lot, medium, little). Drivers reported having turned the siren on when required by the doctor or to ask for opening space in traffic (that´s why the incidence of ´sometimes´ answer was high - N = 24). From the 18 drivers who reported discomfort by siren noise, 11 of them classified it as discomfort, and from those 8 of them belonged to ER hospital. Although there was no significant statistical difference to the category ´monthly use of ambulance´ (p = 0.003), in which drivers from HCFMUSP use it more often than drivers from ER, this did not mean that drivers from HCFMUSP feel more discomfort with siren noise (N = 3). The higher the number of drivers using an ambulance (not matter the hospital), the higher the reference to much discomfort with siren noise will happen (Discomfort grade X monthly use of ambulance, p = 0.042 - Table 4). Experience reports from these drivers showed they are aware of their responsibility in saving lives.
We analyzed right and left ears of ambulance drivers from both hospitals (HCFMUSP and ER). 50% of them presented Costa´s classification 1 to 5 in right and left ears (N = 14, respectively). This percentage is similar to the one by Rossi (1999). Table 3 did not present significant statistical difference (p = 1.000), what showed us there was no predominance of hearing loss of left ear over right ear.
From the 28 examined drivers, we noticed that 14 (50%) with hearing loss according to Costa´s classification (1988) had been working for more than 10 years. Though, 14 individuals (50%) from the group with no signs of noise-induced hearing loss (COSTA´s 0 and 5) who had worked from 1 to more than 10 years, 11 of them had been working as drivers for 10 years at least. The same type of noise (urban one, in this case) could affect the same individuals but in different ways even if they had worked for the same period of time, developing or not hearing loss (Linden, 1996).
We found that 21 individuals (75%) did not make use of air conditioning or air circulator during work. From those, 10 individuals had hearing loss grade 1 to 4 according to Costa´s classification (1988) and 11 of them presented 0 and 5. From the individuals who reported having used air conditioning or air circulator, four of them had Costa´s classification 1 to 4 and three 0 and 5, though they reported having used air conditioning and air circulator very little. This justifies the fact that 100% of drivers answered during anamnesis that they drive their ambulanced with open window. Their excuses were the following: heating, ventilation, avoiding contamination from patients, easy way to ask for way in the traffic and even security (lack of maintenance on ambulances).
We can conclude that the fact drivers drive their ambulances with open window, allowing in this way closer contact between ears and traffic and siren noise, might intensify hearing loss, though 14 individuals had Costa´s classification 1 to 4 (1988) and 14 of them had 0 and 5. Nevertheless, we also noticed that left ear (directly exposed to open window) did not present higher incidence of hearing loss or higher grade than the right ear. Hearing alterations could be influenced by individual´s susceptibility, confirming Linden´s study (1996).
Regarding the 14 individuals with Costa´s classification 1 to 4, seven of them presented recruitment phenomenon. Nevertheless, the higher the number of individuals who did not present recruitment (N=11), the higher the number of hearing incidence with no features of noise-induced hearing loss (Costa´s 0 and 5). The correlation between presence of recruitment and Costa´s classification 1 to 4 (hearing loss occurrence) was considered a significant statistical datum: the pairs of variables "Presence of recruitment X Costa RE" and "Resence of recruitment X Costa LE" presented, respectively, p=0.021 and p=0.001 (Table 4). Recruitment phenomenon occurs by a reduction on dynamic area of hearing, harming emotional, social and professional state of the individuals (Azevedo et al., 1993; Momensohn-Santos and Russo, 2005).
Table 4 shows the correlation between categories studied (questions related to anamnesis) with ambulance drivers from ER and HCFMUSP. We pointed two, among the different pairs of variables whose p was statistically significant. Among the individuals who reported discomfort to siren noise (n=18), there was a positive relation: the higher number of individuals who reported discomfort to heavy sounds, the higher the number of day/month they drove an ambulance. Therefore, the higher the occurrence of the first variable, the higher was of the second one. The second example refers to "Presence of discomfort X Monthly use of ambulance", in which a negative relation occurred: the lower the number of drivers (n = 10) who did not report discomfort to siren noise, the higher the number of day/month they drove an ambulance. Thus, the lower the occurrence of the first variable, the higher was of the second.
Other pairs of variables which were in Table 4 were also important to this study, although there was no significant statistical correlation between the presence and/or grade of discomfort with Costa´s classification (1988) or with the presence of recruitment. We can understand that the presence of hearing loss or recruitment did not influence the presence and the grade of discomfort. On the other hand, the positive correlation between occupation period and reference to discomfort made us think of the influence of non-hearing factors, which affect individuals´ well-being (Corrêa Filho et al., 2002; Balbinot and Tamagna, 2002; Neri, Soares and Soares, 2005; Sanches, 2003; Silva and Mendes, 2005; Souza and Silva, 2005).
CONCLUSIONSWe conclude that:
- The occurrence of Noise-induced hearing loss was 50% (n=14) in this sample, which comprehended drivers from Instituto de Infectologia Emílio Ribas and from Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo;
- There was no significant statistical difference between noise-induced hearing loss on right and left ears;
- Among the individuals who presented noise-induced hearing loss, 35.7% (n = 10) presented recruitment phenomenon.
REFERENCES1. Azevedo AP; Morata TC, Santos UP, Okamato VA Ruído - um problema de saúde publica (outros agentes físicos). In: Buschinelli JTP, Rocha LE, Rigotto RM (Orgs.). Isto é trabalho de gente? Vida, doença e trabalho no Brasil. São Paulo: Vozes, 1993, p.403-35.
2. Balbinot A, Tamagna A. Avaliação da transmissibilidade da vibração em bancos de motoristas de ônibus urbanos: um enfoque no conforto e na saúde. Revista Brasileira de Engenharia Biomédica 2002, 18(1):31-38.
3. Corrêa Filho HR, Costa LS, Hoehne EL, Pérez MAG, Nascimento LCR, Moura EC. Perda Auditiva Induzida por Ruído e hipertensão em condutores de ônibus. Revista de Saúde Pública 2002, 36(6):693-701.
4. Costa EA. Classificação e Quantificação das Perdas Auditivas e Audiometrias Industriais. Revista Brasileira de Saúde Ocupacional 1988, 16(61):35-38.
5. Fiorini AC. O Uso de Registros de Emissões Otoacústicas como Instrumento de Vigilância Epidemiológica de Alterações Auditivas em Trabalhadores Expostos a Ruído. São Paulo, 2000, p.138, (Tese de Doutorado - Universidade de São Paulo - USP).
6. Linden MB. Os conteúdos da consciência do trabalhador exposto ao ruído. São Paulo, 1996, p.147, (Dissertação de Mestrado - Pontifícia Universidade Católica de São Paulo - PUC-SP).
7. Marques SR. Os efeitos do ruído em motoristas de ônibus urbanos do município de São Paulo. São Paulo, 1998, p.118, (Dissertação de Mestrado - Pontifícia Universidade Católica de São Paulo - PUC-SP).
8. Momensohn-Santos TMM, Russo ICP. Determinação dos Limiares Tonais por Via Aérea e por Via Óssea. In: Momensohn-Santos TMM, Russo ICP (Orgs.). A Prática da Audiologia Clínica. 5ª ed. São Paulo: Cortez; 2005, p.67-95.
9. Momensohn-Santos TMM, Russo ICP. Medidas de Imitância Acústica. In: Momensohn-Santos TMM, Russo ICP(Orgs.). A Prática da Audiologia Clínica. 5ª ed. São Paulo: Cortez; 2005, p.206.
10. Momensohn-Santos TMM, Russo ICP. Interpretação dos Resultados da Avaliação Audiológica. In: Momensohn- Santos TMM, Russo ICP(Orgs.). A Prática da Audiologia Clínica. 5ª ed. São Paulo: Cortez; 2005, p.306.
11. Neri M, Soares WL, Soares C. Condições de saúde no setor de transporte rodoviário de cargas e de passageiros: um estudo baseado na Pesquisa Nacional por Amostra de Domicílios. Caderno de Saúde Pública 2005, 21(4):1107-1123.
12. Rossi MM. O perfil audiométrico dos motoristas de ambulância de um Grande Hospital Público da Cidade de São Paulo. São Paulo, 1999, p.75, (Trabalho de Conclusão de Curso do Aprimoramento em Saúde e Trabalho - HCFMUSP).
13. Sanches RG. A Problemática do Ruído Urbano: Descrição e Análise da Literatura. São Paulo, 2003, p.63, (Dissertação de Mestrado - PUC-SP).
14. Silva LF, Mendes R. Exposição combinada entre ruído e vibração e seus efeitos sobre a audição de trabalhadores. Revista de Saúde Pública 2005, 39(1):9-17.
15. Souza NRM, Silva NAS. Exames admissionais e aposentadorias precoces em motoristas de ônibus: influência da hipertensão arterial. Revista da SOCERJ 2005, 18(2):154-139.
1. Mestranda in Speech - PUC-SP (Fonoaudióloga).
2. Doctor of Science in Human Communication Disorders UNIFESP-EPM (Fonoaudióloga the Division of Clinical DSB - HCFMUSP).
3. PhD in Science: Legal Medicine - HCFMUSP (Medical Service of the Occupational Health - HCFMUSP).
Hospital of the Medical School of USP-HCFMUSP.
Mailing address: Gabriela Leite Lopes da Silva - Street Gervásio Pires Ferreira, 120 - Sao Paulo - SP - CEP: 04072-050 - Phone / Fax: (11) 2275-3833 (res.) / (11) 8122-2121 (cel.) - E-mail: gabilopes21@terra.com.br
FUNDAP
This article was submitted in SGP (Management System Publications) in the RAIO 1/5/2006 and approved on 23/5/2006 23:42:58.