INTRODUCTIONThe facial trauma has become an inevitable subject for the medical community for its frequency has been increasing, mainly in the last four decades, and it correlates to the high number of automobile accidents and urban violence (1, 2).
The face, due to its corporal frontal projection, is extremely exposed to aggressions.
Upon being compressed between the bones and the forces of external aggression, the soft tissues may have several lesions (cuts, lacerations, hemorrhages, hematomas etc.) which enable the deleterious effects of the bones fractures (3,4).
The nasal trauma etiology is heterogeneous and the major or minor prevalence of an etiologic factor relates to some characteristics of the population studied (age, sex, social, local, urban and residential classification) (5,6).
In certain regions of our country and in European countries, the use of the bicycle as leisure, sports or a transport means is highly broadcast, which increases the possibility of accidents.
In children and elderly people, the fractures relate to falls at home, child's plays and games (7,8). In young adults, up to the fourth decade, the most common causes, in addition to automobile accidents, are the interpersonal aggressions and traumas resulting from sportive practices (9,10).
Today, the associations of alcohol, drugs, vehicles driving and the increase of urban violence are more and more present as causal factors of facial trauma (11). Most of these lesions occur, mainly, on weekends due to the larger consumption of alcohol for fun and leisure.
Prevention educational campaigns allied to the creation of rigorous laws, such as those of traffic infraction, have tried to change the currently scaring perspectives of accidents with vehicles and urban violence (12, 13).
The objective of this study is to evaluate the relationship between the mechanism of trauma and sex, the frequency of nasal trauma according to the age of the patients and the deviation of the fracture to the right or to the left.
To compare the sex (male and female) to interpersonal violence (aggression).
METHODWe have carried out a prospective study in patients with nasal trauma, who sough this service intentionally, in the period of April through September 2007, in which we evaluated 100 patients of male and female sex, of any age, who had only nasal trauma. Only 86 patients were included in this sample. The excluded were those who had several fractures in the face (frontal, maxillary and mandibular bones) and others who refused to take part in the study.
In the patients evaluation we performed a protocol in which we collected data regarding sex, age, trauma mechanism and nasal pyramid deviation topography after obtainment of free and clear authorization.
In this sample we used non-parametric test of comparison for statistical analysis of the results; the parameters were submitted to chi-square test. We found significance only when the test was applied to both sexes in the age range from 11 to 40 years, the other parameters didn't present statistical significance. The standard deviation was not applied.
The review of the literature was researched through OVID Medline, Pub-Med, Web of Science in English and Portuguese.
This study was approved by the Ethics Committee and research of (UNISA) University of Santo Amaro, under protocol number 057/08.
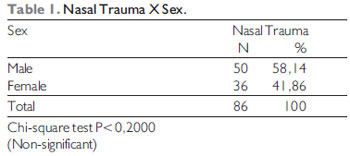
RESULTSThis study revealed the male sex to be mostly affected (58.14%) and the female affection of 41.86% out of a total of 86 patients (Table 1).
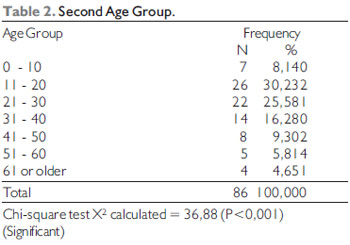
As far as the age group is concerned, the age range from 11 to 40 years had a larger prevalence with significant statistical difference in both sexes X
2 calculated = 36.88 (P<0.001). The group of 61 years of age or more was the least affected (4.651%), followed by the group of 50-60 years (5.814%) and of 0-10 years of age (8.140%) (Table 2).
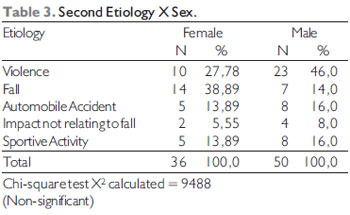
We didn't find statistical significance relating to sex and to trauma mechanism (X² = 9.488), although there is a larger frequency of violence in the masculine group (46.0%) and a decrease in the feminine group (38.89%). As for violence, the male sex (46.0%) prevailed over the female sex (27.78%), and for falls the feminine sex was more affected (38.89%). The automobile accidents occurred more frequently in the masculine sex (16%) and the sportive activities frequency was larger in men (Table 3).
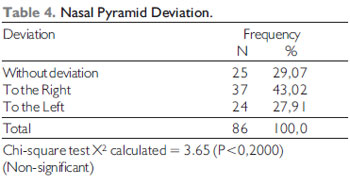
The nasal pyramid deviation to the right or left side didn't appear to be statistically significant, X² calculated = 3.65 (P<0.2000), although the results presented a larger deviation frequency to the right side regarding the face (Table 4).
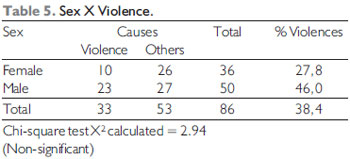
There wasn't either any statistical difference between sex and urban violence X² calculated = 2.94 (Table 5).
DISCUSSIONThe nasal fractures are common diseases caused mainly by automobile accidents, aggressions and falls.
This study suggests a nasal trauma frequency difference between men and women, 58.14% and 41.86% respectively; in spite of no statistical significance, these values were not similar to those of Sherer et al. (14), who, in 788 patients, verified that 80.0% were men and 19.3% were women. The larger frequency in men may be ascribed to the fact they are in a larger number in the traffic, mainly in highway, and practice more contact sports. In women we confirmed the falls are the most frequent causes 38.89%, but without statistical significance, and the literature indicates there is a growing increase of trauma in this group (14). A recent study by Shapiro et al. (20) appointed the automobile accidents as the main cause for severe facial trauma, but the authors justify such fact for the work was performed in a trauma center regional reference institution and this affected the types of traumas the hospital attended as for the severity of the patients. Luce et al. (16) indicated the accidents by automobile vehicles as the main cause for facial fracture (65.0%). Subsequent studies supported such information (15,21), but the trend of the current studies is to show an increase in the incidence of violence and suggests this is the main etiology in the face traumas (19, 12). In this study, the interpersonal violence seems to be the most common cause in men while the automobile accidents contributed for 13.89% in the female sex and 16.0% in male sex, but without statistical significance.
The use of seat belt by drivers of automobiles and helmets by motorcyclists reduced the frequency and severity of the facial lesions followed by traffic accident (13,21,22,23). Speed control rigorous laws, mandatory use of seat belt and air-bag, when applicable, are credited for the decrease in the number of facial fractures due to automobile accidents (12).
The association of alcohol consumption and facial fractures is well documented (11) and Shapiro et al. (20) describe a relationship of up to 45.0% of the cases. A law increasing the age for release of alcoholic consumption with rigorous control, punishment for drunk drivers and a larger social alert about the morbidity relating to alcohol may reduce any traumas resulting from use.
More recently a decree was published in the Official Gazette on June 20, 2008; the law changes provisions of Law no. 9503, of September 23, 1997, that establishes the Brazilian Traffic Code, aiming at setting forth alcoholemia zero and imposing more severe penalties for the driver who drives under the influence of alcohol, which is a crime (24).
Information from 14 units of (SAMU) Emergency Mobile Service published by the Ministry of Health indicates a reduction of 24% of rescue operations since the beginning of the effectiveness of the so-called Dry Law. Therefore, the General Coordination of Urgency and Emergency of the Ministry of Health evaluates the new law has brought an operational improvement to the service with a significant reduction of accidents (28). And the incidence of nasal trauma by automobile accident must decrease considerably.
In this study there was a significance among the age groups; when compared to the occurrence of nasal trauma the most affected age range varied from 11 to 40 years. Wulkan et al (25) confirmed that until 19 years of age, the main cause of facial trauma is fall and most fractures were isolated, mainly of teeth (45.0%) and nose (25.0%). Shaikh et al. (26) reported 7.8% of facial trauma in this age range. In children and adults above 60 years of age, the fractures are less frequent. Posnik (8) and Lucht (7) verified that the low incidence of trauma in these age ranges is due to the family attention, the remaining at home, the childhood cares and the own characteristics of the elderlyly people, such as less activity. In these age ranges, the traumas are simple low impact fractures and they relate to domestic accidents such as slipping, stairs falls and childhood's games.
From 15 to 19 years with the early consumption of alcohol and the involvement with interpersonal violence, approximately half of the traumas result in some type of fracture (30).
From 20 to 39 years, Wulkan et al (28) present the interpersonal violence as the main cause of trauma followed by falls and in older than 40 years, the fall as the main trauma mechanism (62.0%) due to the association with comorbidity (osteoporosis, faintness, vascular brain accident etc.).
Other associated factors such as the use of other drugs, the family frailty and fragmentation, unemployment were difficult to obtain in this record. Many patients would arrive hours, days or months after the trauma, and often omitted the use of alcohol and/or drugs or even information of the accident or aggression.
Such observations confirm those found by Mac Dade et al. (11) that the increase of external violence is due to the current urban society psychosocial characteristics, other socioeconomic and emotional conflicts to which the younger are submitted (9,11,14). The population characteristics, in rural or urban places, the socioeconomic or educational level influence in the etiopathogenesis and the severity of the traumas (5,14). In 1967, Shultz (15) verified that in places of low economic level, the most frequent causes were physical aggression (35.1%), followed by automobile accidents (26.3%) and sports (12.2%). In the more favored places, the main cause was automobile accident. This study was carried out in a low economic level location, with a high level of violence, the South Zone of São Paulo, where the aggressions (interpersonal violence) correspond to 27.78% of the trauma causes in women and 46.0% in men, but there was no statistical significance.
In the sports-related lesions, most of which were associated with collective sports, mainly soccer.
Sherer et al. (14) report that the accidental fractures are mostly caused by relative aggressions (father, mother, husband, son) and associated with the use of alcohol and other drugs (9,11,14).
CONCLUSIONThere was a higher frequency of nasal trauma in the age groups from 11 to 40 years.
In both sexes there was no statistical difference between the female and male sex regarding the nasal trauma.
There was no difference in the trauma mechanism or in the nasal pyramid deviation type in our sample.
BIBLIOGRAPHICAL REFERENCES1. Braustein PW. Medical aspects of automotive crash injury research. JAMA. 1957, 163:249-55.
2. Bull JP. Disabilities caused by road traffic accidents and their relations to severity. Acrid Anal Prev. 1985, 17:387-97.
3. Nahum AM. Biomechanics of maxillofacial trauma. Clin Plast Reconstr Surg. 1975, 2:59.
4. Strula F, Absi B, Buquet Jr. Anatomical and mechanical considerations of craniofacial fractures. An experimental study. J Plast Reconstr Surg. 1980, 6:815.
5. Larsen OD, Nielsen A. Mandibular Fractures: 1- An analysis of their etiology and location in 286 patients. Scand J Plast Reconstr Surg. 1976, 10:213.
6. Tong L, Bauer RJ, Buchmari SR. A current 10-year retrospective survey of 199 surgically treates orbital floor fractues in a non-urban tertiary care center. Plast Reconstr Surg. 2001, 108:612-21.
7. Lucht UA. A prospective study of accidental falls and resulting injuries in the home among elderly people. Acta Soc Med Scand. 1971, 2:105-9.
8. Posnick JC. Pediatric facial fractures. Ann Plast Surg. 1994, 33:442-57.
9. Brook LM, Wood N. A etiology and incidence facial fractures in adults. Int J Oral Maxillofac Surg. 1983, 12:293-8.
10. Bochlogyros P. A retrospective study of 1521 mandibular fractures. J Oral Maxillofac Surg. 1985, 43:597-601.
11. MacDade AM, McNicol RD, Ward-Booth P, Chesworth J, Moos KF. The aetiology of maxillofac injuries, With special reference to the abuse alcohol. Int J Oral Maxilofac Surg. 1982, 11:152-5.
12. Beck RA, Blakeslee DB. The changing picture of facial fractures. Arch Otolaryngol Head Neck Surg. 1989, 115:826-9.
13. Prince JD. Facial fracture and seat belts. Brit Dent J. 1983, 155-12.
14. Sherer M, Sullivan WG, Smith DJ et al. An analysis of 1423 facial fractures in 788 patients at an urban trauma center. J Trauma. 1989, 29:388-90.
15. Shultz RC. Facial injuries from automobile accidents: study of 400 consecutives cases. Plat & Reconstr Surg. 1967, 40:415.
16. Luce EA, Tubb TD, Moore AM. Review of 1000 major facial fractures and associated injuries. Plast Reconstr Surg. 1979, 63:26-30.
17. Convington DS, Wainwright DJ, Teichgraeber JF, Parks DH. Changing patterns in the epidemiology and treatments of zygoma fractures: 10-year review. J Trauma. 1994, 37:343-8.
18. Afzelius LE, Rosen C. Facial fractures: a review of 368 cases. Int J Oral Surg. 1980, 9:25-32.
19. Haug RH, Prather J, Indresano AT. An epidemiologic survey of facial fractures and concomitant injuries. J Oral Maxillofac Surg. 1990, 48:926-32
20. Shapiro AJ, Johnson RM, Miller SF, McCarthy MC. Facial fractures in a level I trauma centre: the importance of protective devices and alcohol abuse. Injury. 2001, 32:353-6.
21. Huelke DF, Compton CP. Facial injuries in automobile crashes. J Oral Maxillofac Surg. 1983, 41:241-4.
22. Johnson RM, McMarthy MC, Miller SF, Peoples JB.Craniofacial trauma in injured motorcyclists:the impact of helmet usage. J Trauma. 1995, 38:876-8.
23. Bachulis BL, Sangster W, Gorrell GW, Long WB. Patterns of injury in helmeted and nonhelmeted motorcyclists. Am J Surg. 1988, 155:708-11.
24. Diário Oficial as União de 20 de junho de 2008, esta Lei altera dispositivos da Lei no 9.503, de 23 de setembro de 1997.
25. Wulkan M et al. Epidemiologia do trauma Facial. Rev Assoc Med Bras. 2005, 51(5):290-5.
26. Shaikh ZS, Worral SF. Epidemiology of facial trauma in a sample of patient aged 1-18 years. Injury. 2002, 33:669-71.
27. Zerfowski M, Bremerich A. Facial trauma in children and adolescents. Clin Oral Invest, 1998, 2:120-4.
28. Ministério da Saúde, SAMU - Serviço de Atendimento Móvel de Urgência, disponível em http://portal.saude.gov.br/portal/saude, acessado em 18/07/2008.
1. Medical Doctor Medical Residence in Otorhinolaryngology.
2. Doctor's Degree in Otorhinolaryngology. Main Professor - Head of the Otorhinolaryngology department of UNISA.
3. Doctor's Degree in Otorhinolaryngology. Head of the Otorhinolaryngology Discipline of UNISA.
4. Doctor's Degree in Otorhinolaryngology. Head of Laryngology and Nasal Endoscopic Surgery of the Otorhinolaryngology Discipline of UNISA.
5. Specialist in Otorhinolaryngology. Specialist Medical Doctor Coordinator of the Medical Residence in Otorhinolaryngology of UNISA.
Institution: Faculdade de Medicina de Santo Amaro - UNISA. São Paulo/SP - Brazil
Mail address:
Roberto Gaia Coelho Júnior
Al. Franca, 1436 - Apto 13 - Cerqueira César
São Paulo/SP - Brazil - Zipcode: 01422-001
Telephone/Fax: (+55 11) 3082-5301
E-mail: betogaia@bol.com.br
Article received on August 13, 2008.
Approved on September 23, 2008.