INTRODUCTIONThe cranial base tumors are uncommon lesions that are not systematically reported in the medical literature. Therefore, it's difficult to evaluate its actual incidence and consequences on the general population's health. Chondroblastoma is an uncommon highly destructive cartilaginous benignant neoplasm, that appear specifically in the long bones epiphysis in young patients (1). Its occurrence is extremely rare in the cranial base, and normally affects the temporal bone (2,3).
We described an uncommon case of a patient presenting with sphenoid bone chondroblastoma that invaded the middle cavity, and was submitted to a successful surgical resection without recurrence after 18 months.
CASE REPORTW.J.S, 37 years old, male, leucodermic, with persistent and strong otalgia for about 3 months. He presented with normal otoscopy, without visible tumorations, with moderate pain at buccal opening. The (CT) computerized tomography confirmed tumor mass in the left infra-temporal cavity, invading the middle cerebral cavity (Picture 1). We carried out intra-oral incision biopsy in the left upper gengivolabial groove, whose histological analysis suggested giant cells tumor.
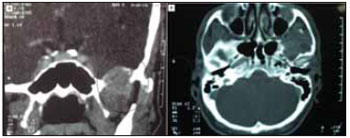
Picture 1. Computerized tomography, coronal (A) and axial (B) cuts, presenting tumor mass in the left infra-temporal cavity, invading middle cerebral cavity, without commitment of the temporal bone (circle).
He was then submitted to micro-surgical resection by frontal approach via orbitozygomatic osteotomy. During the surgery, tomographic statements were confirmed, and no involvement with the temporal bone was found. Wide surgical resection carried out. There were no complications. He was discharged on the 5th postoperative day. The histopathological exam confirmed chondroblastoma (Picture 2).
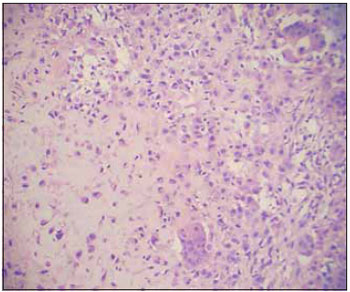
Picture 2. Histological cut confirming chondroblastoma diagnosis (hematoxylin-eosin, 200X).
The patient remains under service follow-up, with quarterly checks and six-monthly CT. After 2 years from surgery, he does not present any complaints, without motor, sensitive or cranial nerves losses, and without recurrence signs in the CT.
DISCUSSIONThe chondroblastomas represent less than 1% of all primary bone tumors. They consist of chondroblasts that are epiphyseal primitive, round or oval cells that contain a dense eosinophilic cytoplasm. The cellular areas are surrounded by variable amounts of dense eosinophilic matrix and may contain calcifications. Mitotic figures and cellular atypias are uncommon. The cystic alterations may simulate aneurismatic osseum cysts (1).
In 1931, Codman (4) ranked it as a chondromatous variant of giant cells tumor when he described these lesions in the proximal humerus. One decade after, Jaffe and Lichtenstein (5) renamed it as chondroblastoma to emphasize the lesion chondroblastic origin and to distinguish it from the classical giants cells tumor.
In long bones, it occurs more commonly between 10 and 30 years old, in a male:female ratio of 2-3:1. There may occur pathologic fractures and, rarely, malignant transformation. Without surgical excision, the tumor may expand to adjacent tissues and metastasize into distant organs. In this region, there is a recurrence of approximately 10% of the cases after surgical removal, the choice treatment (6).
In the cranial base 63 cases were so far described in the temporal bone and 8 in the mandibular condyle (3,4). No description of its occurrence was found isolated in the sphenoid bone.
Indications for surgical removal of tumors from the cranial base has been evolving. Symptoms and live expectation of the patient, the disease natural history and the structures involved by the tumor must be considered during the therapeutic decision. In the case of chondroblastoma of the cranial base, there are only a few pieces of information on therapy and prognosis. In the temporal bone, we suggest that a wide surgical resection promotes a lower recurrence rate (3,4). In this case, we opted for a wide resection since the tumor did not invade important structures such as temporal bone, temporal-mandibular joint and internal carotid artery.
CONCLUSIONSWe described an uncommon case of sphenoid bone chondroblastoma that occupied the infratemporal and middle cerebral cavities. The patient was submitted to wide surgical resection, without recurrence after 2 years.
We remark the importance of the chondroblastoma differential diagnosis, as well as its therapeutic approach, is remarkable in the cranial base lesions, whose objective must always be as wide a resection as possible with the maximal function conservation.
BIBLIOGRAPHICAL REFERENCES1. Turcotte RE, Kurt AM, Sim FH. Chondroblastoma. Human Pathol. 1993, 24(9):944-9.
2. Kurokawa R, Uchida K, Kawase T. Surgical treatment of temporal bone chondroblastoma. Surg Neurol. 2005 Mar, 63(3):265-8.
3. Gaudet EL Jr, Nuss DW, Johnson DH Jr, Miranne LS Jr. Chondroblastoma of the temporal bone involving the temporomandibular joint, mandibular condyle, and middle cranial fossa: case report and review of the literature. Cranio. 2004, 22(2):160-8.
4. Codman, EA. Epiphyseal chondromatous giant cell tumors of the upper end of the humerus. Surgery, Gynecology and Obstetrics. 1931, 52: 543-8.
5. Jaffe HL, Lichtenstein L. Benign chondroblastoma of bone: a reinterpretation of the so-called calcifying or chondromatous giant cell tumor. Am J Pathol. 1942, 18:969-91.
6. Ramappa AJ, Lee FYI, Tang P. Chondroblastoma of bone. J Bone Joint Surg. 2000, 82A(8):1140-5.
1. Resident Doctor of the Otorhinolaryngology Service of the Medicine College of the Federal University of Uberlândia.
2. Otorhinolaryngologist. Head of the Craniomaxillofacial Surgery Division of the Otorhinolaryngology Service of the Medicine College of the Federal University of Uberlância.
3. Doctor. Neurosurgeon of the Neurosurgery Service of the Medicine College of the Federal University of Uberlândia.
4. Master's degree. Head of the Head and Neck Surgery Division of the Otorhinolaryngology Service of the Medicine College of the Federal University of Uberlância.
5. Head Professor. Head of the of the Otorhinolaryngology Service of the Medicine College of the Federal University of Uberlândia.
Institution: Serviço de Otorrinolaringologia, Faculdade de Medicina, Universidade Federal de Uberlândia. Uberlândia / MG - Brazil.
Mail address:
OTOFACE - Rua Arthur Bernardes, 555 - 1º andar
Uberlândia / MG - Brazil - Zip code: 38400-368
Telephone/Fax: (+55 34) 3215-1143
E-mail: lucaspatrocinio@triang.com.br
Article received on October 16, 2007.
Approved on May 21, 2008.