INTRODUCTIONThe increase of live expectation, secondary to the lowering of mortality and birth rates, has made the population aging a fact confirmed worldly, even in developing countries including Brazil. Aging represents simultaneously a triumph of mankind and one of its hardest challenges (2).
The population aging brings deep changes to all sectors of society, but it's in the health area that the strongest transformations are confirmed, specially for they require new resources and structures (2).
There are large differences between elders. Some may remain healthy and with their functional capacities preserved. Others, however, acquire incapacities that may critically affect their quality of life and need specific rehabilitation evaluations and processes, including the use of prostheses and orthoses (3).
Among the losses that occur in the aging process, that affect critically the quality of life and need rehabilitation by means of prostheses and therapy, is presbycusis. Despite it starts about the 30 years old, most individuals begin to present the first audiometric changes at about 50 years old (4). The hearing loss resulting from aging implies environmental factors, to which the individuals are exposed and that may stress this loss degree. Some of the factors are: noise exposure (occupational or not); use of ototoxic medicines; traumatisms; metabolic and circulatory changes; infections (5).
The percentage of elders who presented with hearing loss described in the literature is very variable. National researches present values from 32.2% (1) to 89.23% (6).
The hearing loss is generally bilateral of neurosensorial type, that is, resulting from changes in the functioning of the inner ear (cochlear) or auditory nerve (VIII cranial pair). The degree of hearing loss found in most cases is from slight to moderate (7). The decrease of hearing sensitivity is followed of a loss in the capacity to understand the speech in noisy environments; decrease of the capacity to find the sound source; slowness in the central auditory processing of auditory stimuli (8). The difficulty of speech understanding, in noisy places, must be explained also for the difficulty of elders to pay attention to a determined stimulus (selective attention), due to an inhibition impairment (difficulty to focus the attention to a subject and inhibit irrelevant information) (9).
There are factors that increase the probability for an individual to present with presbycusis, such as age, sex (male), the occupation and the education level (10).
Despite its high prevalence, and the fact of being deemed to be a public health problem (8), the hearing loss in elders is not in the list of problems inquired by doctors, in this age range (11). Some reasons may be the absence of specific complaint, by elders and their families, and the false idea that the elder "listens only when he/she wants", generally found in cases of slight degree hearing loss or a hearing loss limited to high frequencies.
Faced with this reality, we opted to carry out this study, aiming at verifying if there is a relationship between the complaint and the presence of hearing loss in a group of elders living in a neighborhood in the city of Canoas, RS.
METHODThis cross-sectional and observational study was carried out within an interdisciplinary project of elder people evaluation in the Neighborhood São Luís, en Canoas (RS), involving Phonoaudiologist and professors of the courses of Nursing and Physical Education.
The neighborhood mentioned is located at the margins of BR-116 and has an approximate population of 4500 people. Initially, we defined its geographical limits, by means of a search on the current map of the city. Then, professionals and students visited all houses of the neighborhood, in order to identify in which the elders lived. After being identified, they were invited to take part in the research. Those who accepted signed the Free and Clarified Authorization Term and, then, responded to a demographic questionnaire with personal and health information. They were submitted to interdisciplinary evaluation that included research of airway auditory threshold, strength and balance evaluation, quality of life, pain and depression.
As far as hearing function is concerned, the elders were questioned about the complaint of hearing loss as follows: within the demographic questionnaire, there was a list of health problems, which was read by the examiners. They prompted the elder to identify their problems, immediately after presentation of each one of the problems. Among the health problems listed, we included hearing loss.
Before the auditory threshold survey, we made meatoscopy to verify for the presence of obstructing wax in the external auditory conduct, using the otoscope Welch Allyn. In the sequence, we measured the level of environmental noise (Minipa decibelimeter), and verified which room of the house was the most silent for the research of airways auditory thresholds. This was done by using the Interacoustics Audiometer, model AS 208. The elders were positioned with their back turned to the examiner and instructed to raise their hand every time they heard the sound produced by the audiometer. We used the ascendant method (from an inaudible to an audible sound), with a modulated pure-tone (warble), and we took note of the lowest value in which the individual signalized he/she was hearing. The results were registered in an audiogram. The airway auditory thresholds were researched in the frequencies of 250Hz to 8000Hz.
For the results analysis, we used the classification of World Health Organization (WHO), that uses the calculation of the averages of frequencies of 500H to 4000Hz. If the average value is between -10dBNA and 25dBNA, the individual presents normal auditory thresholds; between 26dBNA and 40dBNA, he/she is classified with slight hearing loss; between 41dBNA and 60dBNA, moderate hearing loss; between 61dBNA and 80dBNA, severe hearing loss; above 81dBNA, profound hearing loss. For classification, we always use the values obtained in the best ear (12).
The age descriptive analysis was carried out by means of averages and standard-deviation calculations. For the variables presence and degree of auditory loss the absolute frequency was calculated.
The statistical analysis was executed in the SPSS for Windows. The tests were carried out the two-tail test, and admitted as statistically significant the values of p lower than 0.05.
The project was approved by the Ethics Committee in Research of the University (Protocol 2006/035h).
RESULTSWe identified 72 elders in the neighborhood, but only 50 took part in the evaluations: 35 (70%) women and 15 (30%) men. The average age was of 69.73 ± 7.00 years.
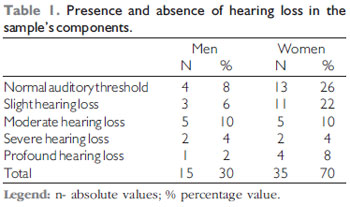
In the interview, only 12 (24%) elders mentioned difficulty to hear. Out of whom, 5 (10%) were men and 7 (14%) were women. However, the data analysis confirmed that 66% had some degree of hearing loss, as described in the data of Table 1.
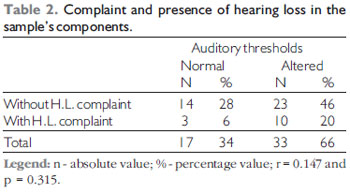
Table 2 describes the data regarding the complaint and the presence of hearing loss among the components of the sample. The statistical analysis didn't make evident a statistically significant correlation, that is, there was no relationship between the presence and complaint of hearing loss in the sample's components.
DISCUSSIONThe presence of hearing loss is a natural consequence of the aging process. It reaches extremely high indexes in individuals of both sexes. Therefore, it would be mandatory to every professional responsible for elders to forward them to auditory evaluations periodically, once even slight degree hearing loss may cause devastating effects in the communicative process, and influence the quality of life of their carriers.
The data analysis showed that, in spite of the low percentage (24%) of complaint of hearing loss, out of the 50 (100%) elders evaluated, only 17 (34%) presented normal auditory threshold: 4 (8%) men and 13 (26%) women.
The index of hearing loss complaint was far lower to that obtained in another study, whose researchers confirmed that 70% of the elders interviewed and assessed declared to have difficulties to hear (13).
The presence of hearing loss in 33 (66%) elders proved to be higher in national (1, 7) and international (14) studies and similar to another national study (15). Although it was carried out in the same city of the only study of population base achieved in Brazil, the values obtained were lower than this, because in the study mentioned a prevalence of 81.2% of hearing loss in elders was confirmed (16). Such information may probably be explained for the size of the sample of this research.
As for the degree of hearing loss, we confirmed that most elders evaluated presented slight and moderate hearing loss, similarly to that described in the literature searched (1, 6, 7, 17). We believe this may explain the inexistence of a relationship between complaint and presence of hearing loss in the sample's components.
For they present with lower degree hearing loss, that allows for the detection of environmental sounds and the speech understanding, specially in silent environments, many times the elders may not perceive they already have hearing changes. Moreover, many individuals with such degrees of hearing loss consider themselves distracted or inattentive and state that, when they concentrate, they understand what is said to them.
We believe that, in such moments, the elders put themselves in a more attentive situation and stand in manner more prone to communication (in front of the interlocutor, diminishing the environmental noises, such as television and radio, making orofacial reading, for instance). In addition to this, the general increase of the speech intensity by the interlocutor. Therefore, the elders obtain a larger number of hints that enable them to understand better. Then, the own elder and his or her relatives begin to believe that he or she hears well, but is very distracted.
The data presented in this study reinforce the need for forwarding the elders for audiologic evaluation, even when there is no specific complaint. Such attitude, by the doctors and other professionals who work with this population, is essential, since the hearing loss affects seriously the individuals' communicative capacity, causes social and family withdrawal, generates isolation and is associated to the depressive pictures aggravation.
Another data to be remarked is that the evaluation must be followed of rehabilitative processes, when necessary. Because in most cases the hearing loss is of neurosensorial type, the forwarding for selection and fitting of hearing aids becomes crucial. Assess and diagnose are no use if they do not provide the elder person with possibility of rehabilitation that will lead to an improvement of his or her quality of life and a better family and social integration (8, 17, 18).
CONCLUSIONThe accomplishment of this work allowed us to verify that among the elders evaluated there was no relationship between the complaint and the presence of hearing loss. Therefore, we emphasize the need for performance of auditory evaluations in all elders in order to also enable them the access to rehabilitation and improve their quality of life.
BIBLIOGRAPHICAL REFERENCES1. Baraldi GS, Almeida LC, Borges ACC. Evolução da perda auditiva no decorrer do envelhecimento. Rev Bras Otorrinolaringol. 2007, 73(1):64-70.
2. Pereira RJ, Cotta RMM, Priore SE. Políticas sobre envelhecimento e saúde no mundo. In: Pessini L, Barchifontaine CP. Bioética e Longevidade Humana. São Paulo: Loyola, 2006. p.289-307.
3. Paschoal SMP. Desafios da longevidade: qualidade de vida. In: Pessini L, Barchifontaine CP. Bioética e Longevidade Humana. São Paulo: Loyola, 2006, p. 329-37.
4. Kasse CA, Cruz OL. Presbiacusia. In: Costa SS, Cruz OLM, Oliveira JAA. Otorrinolaringologia. Princípios e prática. Porto Alegre: Artmed; 2006, p. 430-3.
5. Bilton T, Viúde A, Sanchez EP. Fonoaudiologia. In: Freitas EV, Py L, Neri AL, Cançado FAX, Gorzoni ML, Rocha SM. Tratado de Geriatria e Gerontologia. Rio de Janeiro: Guanabara Koogan: 2002, p. 820-7.
6. Amaral LCG, Sena APRC. Perfil audiológico dos pacientes de terceira idade atendidos no Núcleo de Atenção Médica Integrada da Universidade de Fortaleza. Fono Atual. 2004, 27(7):58-64.
7. Mattos LC, Veras RP. A prevalência da perda auditiva em uma população de idosos da cidade do Rio de Janeiro: um estudo seccional. Rev Bras Otorrinolaringol. 2007, 73(5):654-9.
8. Huang T. Age-related hearing loss. Minn Med. 2007, 90(10):48-50.
9. Parente MAMP, Wagner GP. Teorias abrangentes sobre envelhecimento cognitivo. In: Parente MAMP. Cognição e Envelhecimento. Porto Alegre: Artmed; 2006, p. 31-46.
10. Cruickhanks KJ, Tweed TS, Wiley TL, Klein BEK, Chappell R, Nondahl DM et al. The 5-Year Incidence and Progression of hearing-loss - The epidemiology of Hearing Loss Study. Arch Otolaryngol head Neck Surg. 2003, 129:1041-6.
11. Valete-Rosalino CM, Rozenfeld S. Triagem auditiva em idosos: comparação entre auto-relato e audiometria. Rev Bras Otorrinolaringol. 2005, 71(2):193-200.
12. Organização Mundial da Saúde. WHO/PDH/97.3 Geneva: WHO, 1997.
13. Calas LL, Borges ACA, Baraldi GS, Almeida LC. Queixas e preocupações otológicas e dificuldades de comunicação de indivíduos idosos. Rev. Soc. Bras. Fonoaudiol. 2008, 13(1):12-9.
14. Chang HP, Chou P. Presbycusis among onder chinese people in Taypei, Taiwan: a community-based study. Int J Audiol. 2007, 46(12):738-45.
15. Bilton T, Ramos LR, Ebel S, Teixeira LS, Tega LP. Prevalência da deficiência auditiva em uma população idosa. Mundo da Saúde. 1997, 21(4):218-25.
16. Béria JU, Raymann BCW, Gigante LP, Figueiredo ACL, Jotz GP, Roithmann R et al, Hearing impairment and socioeconomic factors: a population-based survey of na urban locality in southern Brazil. Pan Am J Public Health. 2007, 21(6):381-7.
17. Teixeira AR, Almeida LG, Jotz GP, De Barba MC. Qualidade de vida de adultos e idosos pós adaptação de próteses auditivas. Rev Soc Bras Fonoaudiol. 2008, 13(4):357-61.
18. Teixeira AR, Bós AJG, Souza VBA. A deficiência auditiva e a qualidade de vida de idosos usuários e não usuários de próteses auditivas. In: Teixeira AR. ULBRA Terceira Idade - Envelhecimento no Terceiro Milênio. Porto Alegre: Nova Prova; 2008, p. 163-84.
1. Doctoral Degree in Biomedical Gerontology (PUCRS) Audiology Laboratory Phonoaudiologist / RS.
2. Doctoral Degree in Human Movement Sciences (UFRGS). Professor of the Physical Education Course of the Lutheran University of Brazil (ULBRA).
3. Doctoral Degree in Psychology (Pontifical University of Salamanca). Professor of the Course of Nursing at ULBRA - Canoas / RS.
4. Doctoral Degree in Social Psychology (USP). Professor of the Physical Education Course (ULBRA / RS).
5. Doctoral Degree in Psychology (University of Barcelona). Professor of the Physical Education Course (ULBRA / RS).
6. Doctoral Degree in Phytotechny (UFRGS). Professor of the Physical Education Course (ULBRA / RS).
7. Doctoral Degree in Phytotechny (UFRGS). Professor of the Physical Education Course (ULBRA / RS).
8. Doctoral Degree in Physical Activity and Sports Sciences (University of Leon). Professor of the Physical Education Course (ULBRA / RS).
9. Doctoral Degree in Education (Methodist University of Piracicaba). Professor of the Physical Education Course (ULBRA / RS).
10. Doctoral Degree in Biological Sciences (Neurosciences - UFRGS). Professor of the Physical Education Course (ULBRA / RS).
Institution: Universidade Luterana do Brasil (ULBRA). Canoas / RS - Brazil.
Mail address:
Adriane Ribeiro Teixeira
Praça Dom Feliciano, 26/604 - Centro
Porto Alegre / RS - Brazil - Zip code: 90020-160
Fax: (+55 51) 3211-2058
E-mail: adriteixeira@yahoo.com.br
Article received on January 06, 2009.
Approved on February 25, 2009.