INTRODUCTIONHearing is the sensorial system that helps mankind in the acquisition and development of the oral language and enables their insertion into the socio-cultural environment. The presence of different types and degrees of auditory deficiencies may impact the development of language (1) and thus the social, education and professional insertion.
Due to the impact of the hearing impairment for the development of children, an epidemiological nature research is required aiming at knowing the magnitude of the hearing problems of each city, state and country. Therefore, it may provide the data managers with planning data, performance and evaluation of prevention actions, control and treatment of such problems, as well as help the identification of etiological factors (2).
The World Health Organization notes the hearing impairment affects 250 million of people worldwide, and it is the most frequent sensorial deficit in the populations (3) with prevalence of 2.1% to 8.8% of incapacitating hearing impairment in developing countries (4).
The estimate is approximately 62 million people of the world population aged younger than 15 years have permanent hearing loss, and two thirds, about 41 million, live in developing countries. In neonates the incidence of hearing loss is of 1.5 to 5.95 per 1000 births. In the United States, 1:1000 presented severe auditory loss, while 5:1000 infants presented with moderate auditory loss (5).
According to the Ministry of Health (6) about 30 geographical regions offer 14930 stations where auditory selection programs are installed.
Studies show a rate of service coverage for neonates of 71.52%, in the state of Bahia, 81% in Santa Catarina, 62%, 15% and 32.2% in the states of Sergipe and Paraíba and in the Federal District, respectively (7).
It is by means of such auditory selection programs that the early detection (right after birth) of hearing impairment and its intervention are possible. The prevalence of neonatal hearing impairment observed in a study at the Maternidade de Barbara Heliodora, in Rio Branco, was of 1:200 newborns, with an occurrence rate higher than other diseases selected in the maternity (8).
In Brazil, a population base study, carried out in the city of Canoas (RS) (9), confirmed 21.6% of the population with some degree of hearing impairment, and 6.8% with incapacitating hearing loss (moderate, severe and profound), with a higher prevalence from 60 years of age, in men and with a lower education level. In the pediatric population, the presence of 5.2% of children from four to nine years old and 2.1% from ten to 19 years old with incapacitating hearing loss (above 31 or 41 dB) and 6.8% aged from four to nine years and 4.9% from ten to 19 years with light hearing loss (26-30dB or 40dB) was confirmed. Another study with this population base methodology was carried out in Monte Negro (RO) (10), that detected the prevalence of 2.78% of the population with incapacitating hearing loss and no incapacitating hearing loss was found in children and adolescents from four to 19 years old. The light auditory losses had an occurrence of 7.5% in the children from four to nine years and of 6.67% between ten to 19 years old.
Another research of diagnostic nature carried out in Ceará points out the prevalence of 4.2% of hearing loss in children aged from six to ten years (11). A research performed with 150 children from five to ten years old confirmed the presence of auditory changes in 38%; 63% of the cases presented bilateral hearing loss and 37% presented unilateral hearing loss (12).
This study was carried out in the city of Itajaí, that, according to the Brazilian Institute of Geography and Statistics (IBGE, 2007) (13), presents a population of 163218 inhabitants, amongst whom 38784 children aged up to 14 years, distributed in tax assessment sectors.
Itajaí is characterized as a port and coastal city in the south of Brazil. The vicinity with the sea, the climate and humidity may be triggering factors that contribute for the transmission of viruses and bacteria that cause infectious processes in the upper airways and consequently of hearing problems.
Since 2005, the city has an Auditory Health Attention Service, located in the Universidade do Vale do Itajaí (UNIVALI), which attends the population of 53 cities. Due to the characteristics of the population forwarded to the service, with male sex and elderly prevalence, a group of researchers from the phonoaudiology and otorhino-laryngology area of this Institution sent and approved, in 2007, a research design named "Prevalence of Hearing impairment in the City of Itajaí". Such research followed the population base methodology, proposed by the World Health Organization and its field research occurred in the period from July through December 2008.
In this context, the objective of this research was to characterize the hearing of the children evaluated in the population base study performed in the City of Itajaí / SC.
METHOD This research project was approved by the Ethics Committee in Research of Univali, under authorization no. 206/2008.
The population of this research consisted of dwellers of the urban area of the city of Itajaí (SC), who composed a contingent of 1632183. The size of the sample was calculated by from an estimate prevalence of hearing impairment of 10% with precision of 1.4%, confidence interval and design effect of 2.0. The sampling computing was made in the EPI-INFO 6 program and to determine how many people should be evaluated by census sector 10% of whom were chosen by lot and the computed sample was divided by the number of sectors assorted in order to determine how many individuals should be evaluated in each sector.
Based on this methodology, the researchers evaluated 499 people, out of whom 215 belonged to incomplete houses and 284 to complete houses. Incomplete houses mean those in which one or more people living in the residence were not present in at least three visits of the researchers' team.
Therefore, the sample of this research consists of 119 children aged up to 14 years and 11 months (average = 6:26), corresponding to 23.56% of the total population evaluated in the city of Itajaí, SC. Out of 119 children, 72 (60.51%) were from incomplete houses and 47 (39.49) from complete houses.
The field research was carried out from July through December 2008 in the census sectors assorted. To determine the order of visitation of the sector by the researchers' team, after the assorting, these were numerically ordered in a crescent manner. Then, one block and one corner of each sector were chosen by lot. Starting from this corner the fourth, eighth, twelfth house, and so on, were visited until we reached the set number of houses, from the lower to the higher numeration of the left side of the street. In case the block finished before reaching the number stipulated for visitation, the researchers crossed the street and started the visitation by the right side, following the assorting of every four houses.
All individuals living in the assorted houses were included for visitation and audiological evaluation, and people with mental deficiency or incapacity to sign an authorization to take part in the research or dwellers who refused to take part after three attempts were excluded. Collective, commercial and uninhabited houses were also excluded.
The researchers' team set up some strategies so that the habitants of Itajaí (SC) could be receptive to the visit of the researchers and informed in advance about the objectives and purposes of the research. Therefore, in the assorting and setting of residences, project's introduction letters were delivered to all houses one week before visitation. The researchers' team was also identified with the project's badge and t-shirt.
The participants accepted to take part in the research and signed the Free and Clarified Authorization Term approved by the Ethics committee in Research of Univali, which informed about the objectives, benefits and risks of the research.
The study procedures were based on the evaluation protocol of the Deafness Prevalence and Other Auditory Disorders (14). In the beginning of the home visitations we carried out a measurement of the environmental noise level by means of a digital sound pressure meter set Sound Meter 840029. Then the verification of the external acoustic meatus was made, by using an otoscope aiming to check for foreign body, earwax excess or anything that could stop the performance of the audiological procedures. Those who presented with any type of alteration such as earwax excess and tympanic membrane perforation were forwarded for evaluation with the otorhinolaryngologist at the Univali's Auditory Health Attention Service, and the dweller received a card with date and time of such consultation, as well as an explanation on the reasons why it was required. This procedure was followed when the following signs and symptoms were detected: presence of unilateral or bilateral foreign bodies; presence of unilateral or bilateral tympanic perforation; presence of unilateral or bilateral earwax excess (total occlusion of the external auditory meatus); presence of unilateral or bilateral secretion in the external acoustic meatus; presence of any report of acute infection of the upper airways; presence of report of unilateral or bilateral otalgia; presence of hearing loss equal or higher than 30 dB by the average of 1000, 2000 and 4000Hz at least unilaterally; presence of unilateral or bilateral tympanometric curve of types B or C and presence of auditory complaints associated to tinnitus and dizziness.
Those who did not present abnormalities in the middle ear inspection were submitted to research of the acoustic immittance measurements, by using MT10 equipment of Interacoustic. The impedanciometric battery consisted of the static complacency research, maximal relaxation, external ear pressure and middle ear pressure so as to register the tympanometric curve and research the ipsilateral acoustic reflexes in the frequencies from 500 to 4000 Hz.
The tonal auditory thresholds was then made in all dwellers older than four years, by using the manual Audiometer Welch Ally AM 232, and the stimuli were presented by means of TDH 39 phones. The individuals were prompted to raise their hands every time they heard the sound stimuli. The stimulus presentation was started in 60 dB NA, decreasing at every 10 dB NA every time the individual responded to the sound stimulus presented. The thresholds researched were 1000 Hz, 2000 Hz and 4000 Hz and the new test of 1000 Hz was made at the end of the evaluation. In the characterization hearing loss degrees we used the reference from the World Health Organization (WHO, 1997)9, which classifies the average of three air thresholds in children, from 0 to 15dB, considered to be normal hearing, from 16 to 30dB, light hearing loss; from 31 to 60 dB, moderate hearing loss; 61 to 80 dB severe hearing loss and above 81 dB, profound hearing loss.
In the younger children, from six months to three years and 11 months, a behavioral evaluation was composed by the research of the acoustic lid reflex, the location of the sound source and the recognition of simple orders, as protocol 14. These children were also submitted to the research of the transient-evoked otoacoustic emissions (TEOAE) through Otoport equipment. The frequency bands of 1000 Hz, 1500 Hz, 2000 Hz, 3000 Hz and 4000 Hz. The participants who presented responses in three or more frequency bands were taken as present TEOAE and those who had responses in less than three frequency bands had outcomes taken as absent TEOAE.
The data obtained were registered in an individual questionnaire, containing the identification data and audiological evaluation protocol, in which the results obtained by the audiological procedures carried out were registered.
The results analysis was set up from the sample of children aged up to 14 years and 11 months, evaluated in the field research of the Project "Prevalence of Hearing impairment in the City of Itajaí, SC". This analysis aimed at characterizing hearing in children as for age, sex, census sector, TEOAE presence or absence, audiological profile of the sample for frequency researched in the tonal threshold audiometry, degree of hearing loss in the best ear, types of tympanometric curves and presence and absence of ipsilateral acoustic reflexes. This analysis was descriptive, and established the percentage of the variables occurrence.
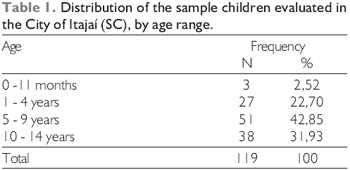
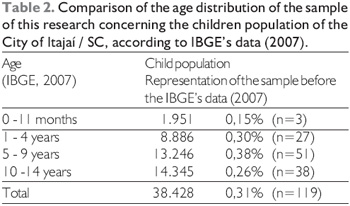
RESULTSIn Table 1 we note the distribution by age range of the sample of children evaluated in the city of Itajaí, SC, with higher prevalence of children older than five years. In Table 2 we observe the proportion of children in the study as for the child population by age range of the city of Itajaí / SC, according to IBGE data (2007) (13).
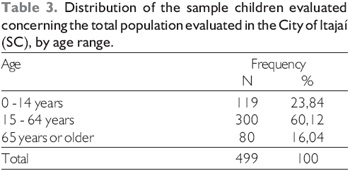
Table 3 confirms that the children represented 23.84% of the population evaluated in the study of the Auditory Prevalence of the City of Itajaí / SC.
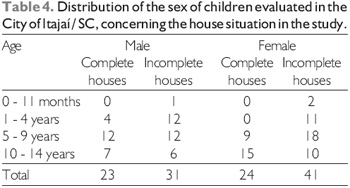
Table 4 describes that 54 (45.38%) of the children were of the male sex and 65 (54.62) of the female sex.
Out of the 119 children, 22 (18.48%) were not submitted to research of the auditory thresholds for being younger than 4 years and in two (1.68%) children aged four years it was not possible to carry out the research for lack of collaboration. Therefore, the audiometric profile of the sample was established with results of 95 children older than 4 years and may be viewed in Figure 1, by means of the average of auditory threshold by frequency researched.
The occurrence of some kind of hearing impairment was of 16.84% in the children older than 4 years, in the analysis of the best ear. Figure 2 describes there was no occurrence of incapacitating hearing loss in the children sample. However, we confirmed a rate of 28.42% of light hearing loss in the right ear (RE) and of 31.58% in the left ear (LE). In Figure 3, we confirmed there was a prevalence (63.42%) of unilateral auditory deficiencies.
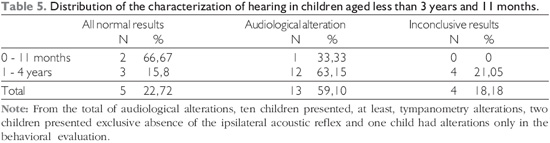
By relating the results of the behavioral evaluation to the tympanometry outcomes, from the ipsilateral acoustic reflexes research and the TEOAE, we confirmed an occurrence of 59.10% of audiological alteration, as in Table 5.
The TEOAE research was made in four of 22 children younger than 3 years and 11 months old, due to the delay in the equipment acquisition, that prevented the return to the houses of eight children. Six children did not help in the TEOAE research and four had the presence of earwax, were suffering from the grippe or with changes in the tympanometry, which prevented the performance of the procedure. Out of four children evaluated, all had present bilateral TEOAE.
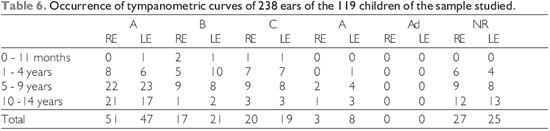
In Table 6 we note that out of the 119 children (238 ears), 52 (21.84%) did not help for the performance of the tympanometry, so that it was made in 67 children (186).
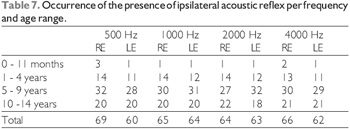
In Figure 4 we observe that the occurrence of absence of acoustic reflexes in at least one of the frequencies researched was very high in both ears. Table 7 presents the number of ears with acoustic reflex present per frequency researched and age range.
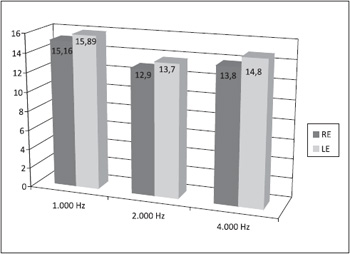
Figure 1. Average of the tonal auditory threshold in the frequencies tested per ear of 95 children of the sample older than 4 years.
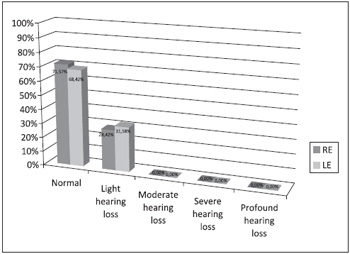
Figure 2. Occurrence of hearing characterization of the sample by the tonal average of the best ear in children older than 4 years.
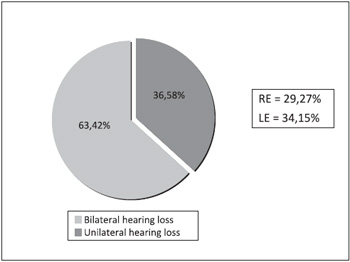
Figure 3. Occurrence of unilateral or bilateral hearing losses in the sample studied.
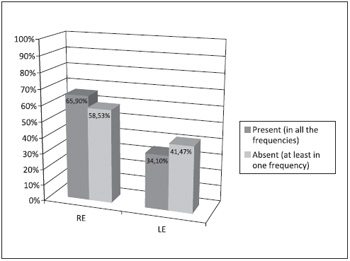
Figure 4. Occurrence of the presence of ipsilateral acoustic reflex per ear.
As for the sample characterization of the children in this study concerning age range, we confirm there were similarities with the distribution of the population of the city of Itajaí / SC, according to IBGE data (2007) (13), with a higher number of children older than five years.
As for the audiometric profile, we may note that, in children over four years, the three frequencies thresholds presented little variation between the very frequencies and ears evaluated, and only in the frequency of 1000 Hz we found thresholds that remained above the normal for the children population (15.16 in the RE and 15.89 in the LE). However, the RE three-tone average was of 13.95 dB and the LE was of 14.79, and were within that exposed by the World Health Organization for the child reference, because the normality analysis must be carried out by the average of the frequencies and not individually (15).
The prevalence of incapacitating (moderate, severe and profound) hearing impairment was not identified in any children, which is opposite to the findings in the city of Canoas (9), that confirmed the presence of 5.2% of children aged from 4 to 9 years and 2.1% from 10 to 19 with incapacitating auditory loss. However, it is similar to the study of Monte Negro (10), that did not either find incapacitating auditory losses in children and adolescents from 4 to 19 years of age.
It is possible that the absence of incapacitating auditory losses in the child population of Itajaí and Monte Negro (10), as well as the minor prevalence in the city of Canoas, in children compared to elderly people, is totally related to the etiological factors of major occurrence of the hearing impairment. In the study of Canoas (9), the most common risk factors were in the male sex, age above 60 years and low education level.
In a study carried out in the State of São Paulo, the external factors were identified to be a cause reported in most occurrences and there was an occurrence of 44% of self-reported hearing impairment in two health queries applied in a population basis (16). Another study performed in the United States indicates smoking, noise exposure and cardiovascular risks as factors contributing to the earlier appearing of hearing impairment in adults (17).
In 1997, a research already pointed out the increase of hearing impairment in three decades, in a city of California, in the United States, indicating that the exposure to noise and ototoxic drugs, such as antibiotics and diuretics are risk factors for the increase of hearing impairment (18). Another etiological factor of high occurrence is presbycusis (19).
In the children population, the most common etiological factor of the hearing impairment is otitis media19, since the consequences on the degree of the hearing impairment are generally from light to moderate.
The occurrence of 16.84% of light hearing impairment in children older than four years, in this research, was higher in the results from Canoas (RS)9, of 6.8% of the children from 4 to 9 years and 4.9% from 10 to 19 years; in Monte Negro (10), from 7.5% of the children aged from 4 to 9 years and of 6.67% between 10 and 19 years; in the native land of Caarapó, in Mato Grosso do Sul, it was of 5.6% (20).
As for children younger than four years, we confirmed 59.10% of occurrence of audiological alteration and 76.92% had tympanometric alterations. Such outcomes point out the conductive hearing impairment as the most prevalent (21).
These results are confirmed by the high occurrence of tympanometric curves type B, C and A (47.32%), as well as the absence of ipsilateral acoustic reflexes in both ears.
As far as the hearing impairment is concerned, in the sample children older than four years, we could confirm a higher occurrence in the left ear (31.58%) than the right ear (28.42%); and there is a concordance with the higher occurrence of unilateral hearing losses in the left ear (34.15%) or of the right ear (29.27%) compared to bilateral hearing losses. Studies report the incidence of auditory alterations in 57 individuals, in whom bilateral hearing loss was identified in 63% and unilateral loss in 37% (12).
CONCLUSIONBased of the results presented, we conclude that the children of the City of Itajaí / SC, when it comes to hearing, present the following characteristics:
- Tonal auditory thresholds average in 1000 Hz of 15.16 dB, in 2000 Hz 12.9 dB and in 4000 Hz 13.8 dB in the right ear.
- Tonal auditory thresholds average in 1000 Hz of 15.89 dB, in 2000 Hz of 13.9 dB and in 4000 Hz 14.8 dB in the left ear.
- 71.57% of the children older than four years with normal hearing in the right ear and 68.42% with normal hearing in the left ear.
- Prevalence of 16.8% of hearing impairment and these had light degree, because there was no occurrence of incapacitating hearing impairment.
- 63.42% of the auditory deficiencies are unilateral and 36.58% are bilateral.
- 22.72% of the children younger than four ears with normal hearing, 59.10% with some auditory alteration and 18.18% with inconclusive results.
- 52.68% of the children had type A curve and 47.32% had type B, C or A curve. 65.90% of the children with ipsilateral acoustic reflexes present in the right ear and 58.53% in the left ear.
Therefore, this research alerts for that in the City of Itajaí, SC, the risk factors for which preventive measures must be taken are those regarding the conductive hearing losses.
ACKNOWLEDGMENTSThe authors thank the collaboration from students Leila Rosso Duzioni, Mariana de Assis Machado, Angelize Guiolo. Fernanda Schultz, Naiara S. Espósito and from the Phonoaudiologist Poliana Sgarbossa, who took part in the field research, as well as FAPESC and Article 170 of the Government of the State of Santa Catarina, for the financial resources granted for accomplishment of the research.
BIBLIOGRAPHICAL REFERENCES1. Gatto IC, Tochetto TM. Deficiência auditiva infantil: implicações e soluções. Rev. CEFAC [periódico na internet]. 2007 jan./mar [acesso em: 2008 Jun. 01];9(1): [aproximadamente 6 p.]. "Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1516-18462007000100014&lng=pt".
2. Rouquayrol Z. Contribuições da epidemiologia. In: Campos GWS, Minayo MCS, Akerman M, Drumond Junior M, Carvalho YM. Tratado de Saúde Coletiva. 2. ed São Paulo-Rio de Janeiro: Hucitec e Fiocruz; 2008. p. 319-373.
3. Mathers C, Smith A, Concha M. Global burden of hearing loss in the year 2000. Global Burden of Diseases 2000. Who. 2000.
4. World health organization. Prevention of deafness and hearing impairment. Disponível em: http://www.who.int/pbd/deafness/en/survey_countries.gif.
5. Guefier,BC, Siqueira M P. O teste da orelhinha. Revista Vida e Saúde. Fev. 2009, 36-7.
6. Ministério da Saúde (MS). Indicadores do programa nacional de triagem neonatal. Brasília (DF): Ministério da Saúde, 2007. Disponível em: http://portal.saude.gov.br/portal/arquivos/pdf/INDICADORES_TRIAGEM_ NEONATAL.pdf.
7. Almeida AM, Godinho TM, Teles MS, Rehem APP, Jalil HM, Fukuda TG, et al . Avaliação do Programa de Triagem Neonatal na Bahia no ano de 2003. Rev. Bras. Saúde Mater. Infant. [periódico na Internet]. 2006 jan./mar. [acesso em: 2009 mar. 03];6(1):[aproximadamente 6 p.]. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext &pid=S1519-38292006000100010&lng=pt&nrm=iso.
8. Borges CAB, Moreira LMO, Pena GM, Fernandes FR, Borges BCB, Otani BH. Triagem auditiva neonatal universal. Arq. Int. Otorrinolaringol. [periódico na Internet]. 2006 jan./mar [acesso em: 2009 mar. 03]: 10(1): [aproximadamente 7 p.]. Disponível em: http://www.arquivosdeorl.org.br/conteudo/acervo_port.asp?Id=352
9. Beria JH, Raymann BCW, Gigante LP, Figueiredo ACL, Jotz G, Rothman R, Costa SS, Garcez V et al. Hearing impairment and socioeconomic factors: a population-based survey of an urban locality in southern Brazil. Rev. Panam Salud Pública 2007, 21(6): 382-387.
10. Bevilacqua MC, Costa OA, Raymann BW, Alvarenga KF, Moret ALM, Banhara MR, et al. Population based survey on ear and hearing disorders Monte Negro, RO Brasil. Relatório final. São Paulo: Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) e reitoria de cultura de extensão - Universidade de São Paulo, 2006 mar.
11. Faria LAQ, Carvalho WSG, Antunes DK. Prevalência e fatores de risco associados a problemas fonoaudiológicos nas crianças da comunidade de Dendê. Rev Pediatr [periódico na Internet]. 2008 jan./jun [acesso em: 2008 dez. 12]: 9 (1): [aproximadamente 6 p.]. Disponível em: http://www.socep.org.br/Rped/pdf/9.1%20Art%20 Orig%2001%20%20Preval%C3%AAncia%20e%20 fatores%20de%20risco%20associados%20a%20problemas%20 fonoaudiol%C3%B3gicos%20nas%20crian%C3%A7as%20 da%20comunidade%20do%20Dend%C3%AA.pdf.
12. Guida HL, Diniz TH. Perfil audiológicos em crianças de 5 a 10 anos de idade. Arq. Int. Otorrinolaringol.[ periódico na Internet]. 2008 abr./jun [acesso em: 2009 mar. 03]: 12(2): [aproximadamente 9 p.]. Disponível em: http://www.arquivosdeorl.org.br/conteudo/acervo_port.asp?id=518.
13. Ministério do planejamento, orçamento e gestão. População recenseada e estimada, segundo os municípios - Santa Catarina - 2007. Brasília (DF): Instituto Brasileiro de Geografia e Estatísticas (IBGE). Disponível em: http://www.planejamento.gov.br/noticia.asp?p=bsc
14. Ministério da Saúde (BR). Manual de instruções: parte geral. Brasília (DF).
15. Santos TMM, Russo ICP, Borgianni LM. Interpretação dos resultados da avaliação audiológica.In: Santos TMM; Russo ICP. Prática da audiológia clinica. 6 ed. São Paulo: Cortez;2007. p. 293-310.
16. Castro SS, César CLG, Carandina L, Barros MBA, Alves MCGP, Goldbaum M. Deficiência visual, auditiva e física: prevalência e fatores associados em estudo de base populacional. Cad. Saúde Pública. 2008, 24(8):1773-1782.
17. Agrawal Y, Platz EA, Niparko JK. Prevalence of hearing loss and differences by demographic characteristics among US adults. Arch Intern Med. 2008, 168(14):1522-1530.
18. Walahagen MI, Strawbridge WJ, Cohen RD, Kaplan GA. An increasing prevalence of hearing impairment and associated risk factors over three decades of the Alameda Country Study. American Journal of Public Health. 1997, 87(3):440-442.
19. Abdel-Hamid O, Khatib OMN, Aly A, Morad M, Kamel S. Prevalence and patterns of hearing impairment in Egypt: a national household survey. La Revue de Santé de la Méditerranée orientable. 2007, 13(5):1171-1180.
20. Picolli RP, Carandina L, Ribas DLB. Prevalência de hipoacusia em crianças indígenas Kaiowá e Guarani. Rev. Bras. Saúde Mater. Infant. 2006, 6(2).
21. Elahi MM, Elahi F, Elahi A, Elahi SB. Paediatric hearing loss in rural Pakistan. The Journal of Otolaryngology. 1998, 27(6):348-353.
1. Phonoaudiologist. Doctoral Degree in Neurosciences, IPUST, SP. Professor of the Phonoaudiology Course and Specialization in Audiology at UNIVALI / SC.
2. Grant Holder of Scientific Initiation, Art. 170 of the Government of the State of Santa Catarina, UNIVALI / SC. In the Course of Phonoaudiology, UNIVALI / SC.
3. Phonoaudiologist. Master's Degree in Human Communication Disorders, UFSM / RS, Arrangement with EPM/UNIFESP / SP. Professor of the Phonoaudiology Course and Specialization in Audiology at UNIVALI / SC.
4. Graduation at UNIVALI / SC. Universidade do Vale do Itajaí - UNIVALI. Phonoaudiologist.
5. Phonoaudiologist. Doctoral Degree in Sciences (experimental Physiopathology) USP, SP. Professor of the Phonoaudiology Course and Specialization in Audiology at UNIVALI / SC.
6. Otorhinolaryngologist. Auditory Health Attention Service, UNIVALI / SC. Professor of the Course of Specialization in Audiology and Doctor of the Auditory Health Attention Service, UNIVALI / SC.
Institution: Universidade do Vale do Itajaí. Itajaí / SC - Brazil. Mail Address: Sheila Andreoli Balen - Rua Uruguai, 458 - Centro - Itajaí / SC - Brazil - Zip Code: 88302-202 - Telephone: (+55 47) 3341-7589 - E-mail: sheila@sheilabalen.com.br. Financial support: Foundation for Support of Scientific and Technological Research in the State of Santa Catarina (FAPESC). Article received on September 17 2009. Approved on October 13 2009.