INTRODUCTIONSnore has been a frequent complaint in the doctors' consulting rooms, and the discomfort caused by the excessive noise may generate matrimonial conflicts and damage to the patients' social activities. The general complaints of Daytime sleepiness, fatigue, behavioral and cognitive alterations are not much valuated not even by the patient, who ascribes them to physical, emotional wears or aging (1). However, a suitable evaluation may diagnose that the snore is associated to a more severe sleep disorder: the obstructive sleep apnea syndrome (OSAS).
The OSAS is a condition characterized by the repetitive obstruction of the upper airways for a period equal or longer than 10 seconds which frequently results in the oxygen desaturation and sleep fragmentation. The classical manifestation is the daytime sleepiness, but other symptoms such as snore, agitated sleep, low concentration and fatigue are frequently reported (2).
This syndrome is considered to be a public health problem for it causes an increase of traffic and work accidents, as well as cardiovascular morbimortality. In the United States, its prevalence in the general population is of about 9% in men and 4% in women, aged between 30 and 60 years, and it is even higher in the obese population (IMC>30). However, this prevalence may be underestimated because some authors believe that about 95% of the patients with sleep disorder are not diagnosed (3).
Today, the assisted Polysonography (PSG) is the gold standard for the OSAS' diagnosis. In this exam authentic data of the severity of this disease is supplied such as, records of electroencephalogram, electrocardiogram, electromyography, corporal movements, training and sleep continuity, oxymetry, airflow and breathing effort. However, it is an expensive exam of difficult access and even uncomfortable for some patients (4). Some questionnaires were thus created in order to help the diagnosis of patients with high risk of OSAS and evaluate the somnolence of these individuals. Out of some questionnaires used for this purpose, we can mention the Berlin's Questionnaire (5, 6) (BQ) and the Epworth Sleepiness Scale (7) (ESS).
Several studies have been confirming complications associated to the sleep breathing disorders such as: systemic blood hypertension, pulmonary hypertension, metabolic syndrome, increase asthma exacerbations, acute myocardial infarction, cardiac arrhythmia, cerebrovascular accident, etc. (8, 9, 10). Such complications stand out the importance of early diagnosis and treatment of OSAS.
The objective of this study is to analyze the results from the Berlin's Questionnaire and the Epworth Sleepiness Scale completed by the patients admitted at Spa Med Campus Sorocaba, aiming at finding the patients who have a high risk of having obstructive sleep apnea (OSAS) and excessive daytime sleepiness (EDS).
METHOD Transversal study, carried out at Spa Med Campus, Sorocaba, in the State of São Paulo, during the year 2008. We applied questionnaire to all patients who got through the initial medical exam on the admission day. The inclusion criteria were the following: adults, both sexes, admitted in the spa. We left out the cases of incomplete questionnaires. All patients were submitted to general physical and full otorhinolaryngological exam.
The patients answered the Berlin's Questionnaires and the Epworth Scales voluntarily upon admission, and there was interference by the physician only in case of doubts. The Body Mass Index (CMI) was computed according to the weight (Kg) and height (m) of the patients at the occasion.
In the Berlin's Questionnaire, the patient marks only 1 response per question and the ultimate interpretation of the answers suggests whether he/she has high risk of OSAS (positive) or not (negative).
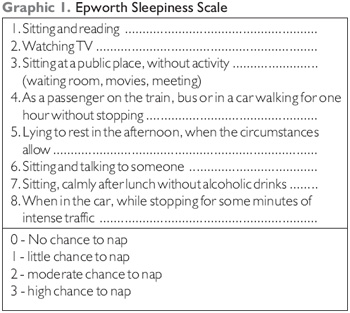
In the Epworth sleepiness scale, the patient sets a mark from 0 to 3 for the chance to fall asleep in each of the 8 situations (Graphic 1). The final sum may vary between 0 and 24 points, and the patients who obtained a score of 10 or more were designated as positive, that is, they had excessive daytime sleepiness. The individuals with final results lower than 10 were classified as negative.
RESULTSWe obtained a total of 276 patients, aged between 18-86 years (Mean age=45 years), with a total of 183 women (66.3%) and 93 men (33.7%). The prevalence of obese (IMC>30) was of 111 patients (40.2%), including 66 women (59.4%) and 45 men (40.6%).
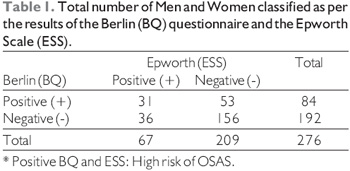
As for the questionnaires results, in the positive BQ group, we obtained 84 patients: 34 men and 50 women. As to the ESS, by taking as positive the patients with score of 10 or over, we found a total of 67 patients (24 men and 43 women), as described in Table 1. Therefore, the association of positive Epworth and Berlin occurred in 14 men and 17 women.
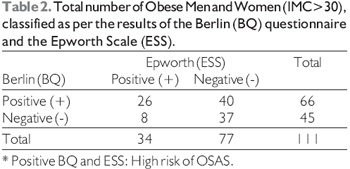
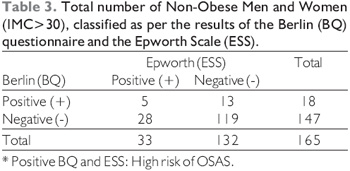
Moreover, we also obtained the ratio between Obese and Non-obese of both sexes, grouped according to the BQ and ESS results, as shown in Tables 2 and 3.
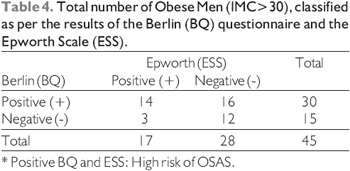
As for the prevalence of obese men who had a high chance to have OSAS, it is described in Table 4.
The concordance coefficient between the questionnaires (BQ and ESS) was Kw=0.19, McNemar Test with x2 calc = 2.87. Among the obese, it was x2=20.02 (P<0.001), which demonstrates a statistical significance with the use of the questionnaires.
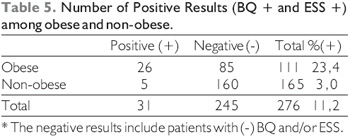
By thus comparing the proportion of positives (BQ and ESS) of obese and non-obese (Table 5), we confirmed a x2=27.679 (p<0.0005) with a high statistical significance.
DISCUSSIONOur study presented the same mean age found in the general population of the literature; but a high prevalence of obese was found (42.2%) and these were mostly of the female sex (59.4%).
Out of these patients, the most prone candidates to undergo polysonography for confirmation of the OSAS diagnosis would the those who had positive (+) BQ and ESS results, summing up 31 patients because they have a high risk of sleep obstructive apnea. From these individuals, 26 (83.8%) are obese, 14 men and 12 women, which shows the high correlation between obesity and OSAS. Out of the male and obese patients, all (100%) had a high risk of OSAS; among the female sex and obese, 70% presented positive results in both questionnaires. This may be grounded on the reduced number of men compared to the number of women in the sample obtained.
Therefore, according to the worldwide literature, 9% of men and 4% of women of the general population have OSAS. According to our data, the men seem to have a major chance to present with OSAS because we found that out of the 93 men of the study, 15% had a high chance to have OSAS, and needed to undergo the polysonography exam in order to confirm the diagnosis; while out of the 183 women, only 7.6% needed to undergo it; therefore, although the total number of women is higher, the final percentage is still lower, as well as it occurs with the general population.
In a preference order, we believe the patients with (+) BQ and (-) ESS would be strong candidates to make PSG. Then the patients with (-) Berlin and Epworth would come, presenting a low risk to have OSAS.
One of the great problems in the OSAS diagnosis is that one of the main symptoms, hypersomnolence, is subjective. In addition to this, there are difficulties in the clinical diagnosis, such as: 1) Snores and somnolence may be minimized or denied by the patient; 2) Snores are normally perceived if there is someone to hear them; 3) Sleep deprivation is becoming common in our society; 4) Progressive somnolence may make the patient get used to an abnormal state of alert 5) There may be difficulty to tell somnolence from fatigue and/or depression; 6) The obesity itself is related to the excessive daytime sleepiness, even in individuals without OSAS diagnosis.
One of the limitations of the evaluation with questionnaires is that it depends upon the sincerity of the patients in the responses and on the self-evaluation subjectivity, and these may result in a discrepancy between the scales and the polysonography. Nevertheless, these questionnaires are still helpful tools to select the best candidates for the polysonography exams, since it is an onerous, hard examination and not all patients are able to undergo it.
CONCLUSIONThe progressive increase of the obesity prevalence in the population contributes for a major prevalence of the associated co-morbidities, such as OSAS, that need to be early diagnosed and treated in order to improve the quality of life of these patients.
The ESS and the BQ have been useful currently for selection of the sleep disorders, specially the OSAS, and may serve as a possible indicator for polysonography. The results from our questionnaires confirm the high prevalence of individuals interned in a slimming spa with risk to have OSAS, specially the group of the obese. The next stage of our study will be to correlate the data obtained with the results of the polysonography.
BIBLIOGRAPHICAL REFERENCES1. Bittencourt LR, Togeiro SMGP, Bagnato MC. Diagnóstico da Síndrome da apnéia e hipopnéia obstrutiva do sono. In: Stamm A. ed. Rinologia. São Paulo: Komedi; 2002: 103-11.
2. Flemons WW, Buysse D et al. The Report of American Academy of Sleep Medicine Task Force. Sleep Related Breathing Disorders in Adults: Recommendations for Syndrome Definition and Measurement Techniques in Clinical Research. Sleep. 1999, 22:667-89.
3. Mercado JC. Identifying Obstructive Sleep Apnea: A Highly Prevalent and Underdiagnosed Disease. Physician Assistant. 2003, 27(2):39-45.
4. Atualização Otorrinolaringológica em Cirurgia de Ronco e Apnéia. Rev Bras Otorrinolaringol. 2002, 68(5) supl.3.
5. Netzer NC, Stoohs RA, Netzer CM, Clark K, Strohl KP. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann Intern Med. 1999 5, 131(7):485-91.
6. Chung F, Yegneswaran B, Liao P, Chung SA, Vairavanathan S, Islam S, Khajehdehi A, Shapiro CM. Validation of the Berlin questionnaire and American Society of Anesthesiologists checklist as screening tools for obstructive sleep apnea in surgical patients. Anesthesiology. 2008, 108(5):822-30.
7. Murray JW. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep. 1991, 14:540-5.
8. Dart RA, Gregoire JR, Gutterman DD, Woolf SH. The Association of Hipertension and Secondary Cardiovascular Disease With Sleep-Disorder Breathing. Chest. 2003, 123(1):244-60.
9. Alkhalil M, Schulman E, Getsy J. Obstructive sleep apnea syndrome and asthma: what are the links? J Clin Sleep Med. 2009, 5(1):71-8.
10. Wenner JB, Cheema R, Ayas NT. Clinical Manifestations and Consequences of Obstructive Sleep Apnea. J Cardiopulm Rehabil Prev. 2009, 29(2):76-83.
1. Post-Graduation (Doctoral Degree) at the Medical School of the University of São Paulo (FMUSP). Coordinator of the Otorhinolaryngology Hospital of Sorocaba/BOS. In charge of the Otorhinolaryngology Service and Sleep Medicine at the Spa Med Sorocaba Campus.
2. 6th-year Medical Student at FCMS PUC-SP Sorocaba Campus. Student
Institution: Hospital de Otorrinolaringologia de Sorocaba/BOS e FCMS-PUC SP Campus Sorocaba. Sorocaba /SP - Brazil. Mail Address: Azis Arruda Chagury - Rua Martinica, 874 - Jd. América - Sorocaba / SP - Brazil - Zip code: 18046-805 - Telephone: (+55 15) 8131-7500 - E-mail: azischagury@gmail.com. Article received on October 17 2009. Approved on November 30 2009.