INTRODUCTIONWith the medicine evolution and technological breakthrough, it has become possible to attain resources to provide hard-of-hearing people with a quality of life. The hearing aid is one of the options in the hearing rehabilitation process, in order to help communication and minimize the several restraining effects caused by this impairment (1).
In the United States, between 10% and 30% of hearing aid users above 60 years of age effectively use the device on a continuous basis, and the rest of this group claims not to use it because of the underestimation of impairment, stigma (2-4), physical comfort of the mold, difficulty in using the telephone, scheduling changes (4), need for supplementary communication strategies and unreal expectations over it.
Even with the technological breakthrough, selecting the hearing aid requires an accurate and clear-sighted process involving procedures, such as choosing characteristics and model of hearing aids, manufacturing auricular molds, deciding about binaural or monoaural adaptation, orientation, esthetical condition, evaluating the expectation level and personal anxiety, as well as tests to verify and validate the adaptation, and a careful individualized assistance (5,6). These procedures are described in a wide range of protocols developed with the objective of maximizing the performance, benefit and the hearing satisfaction (7-9).
The clinical evidences reveal that including general information on the individual's health, history and particular characteristics in this process enables the prognosis and the acceptance to use it (10), making it primarily important that the professional is aware of both the technology and the procedures chosen for the evaluation and adaptation process of the hearing aid (11).
This study had the objective to describe the hearing aid fitting protocol applied to adult and elderly individuals at Audiological Center of Otorhinolaryngology Foundation - Clinic Hospital of the Medical School of University of Sao Paulo. Its preparation was performed by data found in the scientific literature that is specific to the field, and it was supplemented by general information proved by the clinical experience. However, it is taken into consideration that it can vary with the different services.
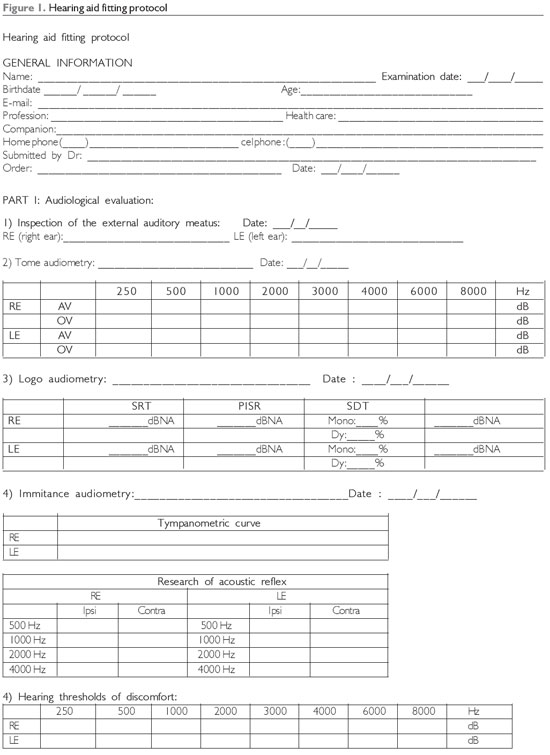
HEARING AID FITTING PROTOCOLThe hearing aid fitting process was comprised of four major parts, according to Figure 1. It is important to emphasize the relevance of guidance and assistance (5,6) based on the information of all the described stages.
Part I - Audiological evaluation
Audiological evaluation is an essential part to characterize the type and magnitude of the hearing loss, indicate the utilization of hearing aid and analyze the individual's expectations, what is fundamental to obtain detailed information. This stage is comprised of the following procedures:
1. Inspection of the external acoustic meatus (EAM): contrary to the medical view, it does not have a diagnostic purpose; it is, however, necessary to verify the excess of serum production and the analysis of the curves of the external acoustic meatus, the individual cannot be a good candidate to the microchannel model, as a consequence of the lack of internal space to assemble or to handle in its insertion or removal.
2. Tone audiometry by airway and osseous pathway: it will help choose the technology, model and electroacoustic circuits required for the individual, when they are added to the information on the physical structure of the external acoustic meatus.
3. Logo audiometry: together with the previous information, this data will contribute to determine the microphone type of the hearing aid, as well as to guide the individual about his/her expectations and hearing performance (12).
4. Immitance audiometry with tympanometric curve and research on acoustic reflex: Tympanometry allows for the analysis of possible alterations in the middle ear that can impact the amplification, and the research of the acoustic reflex allows for the verification of Metz's objective test of recruitment. This data is important when they are added to the hearing thresholds to make the dynamic hearing field to be worked on with sound amplification.
5. Hearing thresholds of discomfort: collection of hearing thresholds of discomfort involving the frequencies of 250 to 8000 Hz will be used to regulate the maximum output of the hearing aid (13).
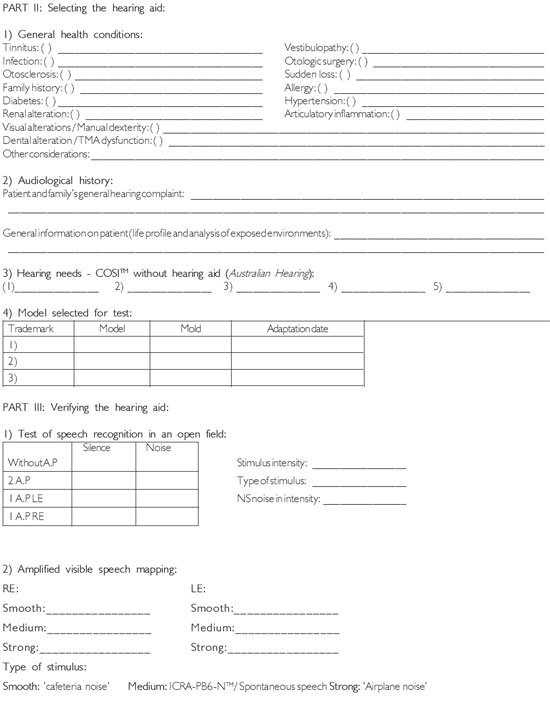
Part II - Selecting the hearing aid
Hearing anamnesis is defined as the individual's previous history, in which it is investigated the cause of deafness, the possibilities of adaptation to the hearing aid and the possible prognoses when using it. In anamnesis, it is intended to attain relevant information with regard to the hearing complaint, individual's general information - including esthetical data, costs and maintenance, as well as information on general health that can interfere with the process. The items of anamnesis are as follows:
1. General health conditions:
- Tinnitus: in cases of hearing loss associated with tinnitus, choice must be made when the degree of loss allows it, by choosing model, technology and mold that will not leave the ear occluded (open earmold or relief venting) (14) and adjusting specific programming, such as expansion deactivation, what enables the frequency of tinnitus. Individuals with tinnitus complaints must receive a careful guidance about the importance of using hearing aids, assistance with respect to the time of stimulation response and the need for a multidisciplinary follow-up to achieve a good prognosis (14).
- Vestibulopathy: when considering that individuals with hearing loss can also suffer from labyrinthic alterations (15), this information becomes essential to the model-selecting process of the hearing aid, the limitation of maximum output, as well as the guidance before stating the home test, since the hearing thresholds can be changed on a temporary or permanent basis.
- Infection: infections recurring from middle and/or external ear can lead to a reduction of the response of the acoustic gain of the hearing aid, as well as possible physical discomforts in the period of infection (16). In case the individual presents in his/her history recurring infections, the model to be chosen must be easily cleaned and maintained, preferably acrylic molds with a lower retention of impurities and easily washable. Obstruction of the external acoustic meatus must be carefully evaluated.
- Otologic surgery (radical mastoidectomy, fenestration): Individuals submitted to surgeries with alteration of the external acoustic meatus should preferably use retroauricular model with an electroacoustic characteristic with an algorithm to cancel microphonia, when configuration of hearing loss enables it. Among the possible difficulties in the molding process, they can be related to the possibility of retaining the mold and/or microphonia due to the irregular characteristic of the external acoustic meatus.
- Otosclerosis: Observation of the conductive or mixed component will help fit the hearing aid, since the intensity perception level in these individuals is different if compared to neurosensorial cases. Due to the alteration in severe frequencies, the individual must be assured to receive the necessary amplification and that the mold is properly fitted so there will not be a loss of sound. The wide dynamic field and the high index of word recognition allow for the prognosis (17).
- Sudden hearing loss: intervention should be started as soon as possible, right after it has been released by the otorhinolaryngologist doctor, thus avoiding hearing deprivation (18). Research of tone hearing thresholds must be performed in the programming adjustors, and it is important to select hearing aids with a wide amplification band for the necessary adjustments.
- Family history: It is estimated that 16% of the cases of deafness in Brazil have confirmed genetic causes (19). Therefore, individuals with previous family histories for hearing loss must be guided and assisted with regard to the genetic component in the family, as well as have a multidisciplinary follow-up to prevent and detect other likely cases.
- Allergy: severe dermatitis in the external acoustic meatus found in some users of hearing aids can be caused by the contact allergy with the material used in the auricular mold - acrylic or silicon (20), and it is important in these cases to submit it to the doctor and a new manufacturing of mold with hypoallergenic material.
- Diabetes: Among their major characteristics, the diffuse thickening of the basal membrane of the vascular endothelium (diabetic microangiopathy) and the neuronal degeneration that can impact the blood irrigation in the cochlea or even cause lesions in the eighth cranial nerve (21). For individuals with diabetes, models with a wide amplification band must be preferably chosen, in order to allow for adjustments if necessary, detailed assistance about the likely benefits and restraints of the hearing performance and request for a new audiological follow-up consultation every six months to check the hearing aid.
- Hypertension: microcirculatory insufficiency can cause a peripheral or central impairment in the hearing and vestibular systems caused by the reduction of oxygen transportation (22). Hearing distinction and/or thresholds can float with pressure oscillations in individuals who do not present a proper control, and, during selection, choice must be made for models with more flexible power adjustment.
- Renal alteration: Increase in the level of urea in the blood of individuals with renal alterations (23), users of hearing aids, can cause damages to the physical structure of both microchannel models, provoking the corrosion of the capsule tip, and the retroauricular models, in which sweat can cause damages to external structures. In these cases, it is important to have an audiological follow-up every six months to check the hearing aid associated with the guidance and assistance with regard to hygiene and maintenance procedures.
- Articulatory inflammation: modifications in articulations caused by pathologies such as arthritis or arthrosis and the choice for a hearing aid of a model with a deeper insertion such as microchannel - in which the internal portion can touch the osseous part of the external acoustic meatus, they can cause a significant physical discomfort and make it no longer be used. For these individuals, a less profound mold or manufactured with a more flexible material allows for more comfort and tolerance in the everyday utilization, besides being more easily handled for its size.
- Visual alterations and/or difficulty in manual dexterity: for these individuals, retroauricular hearing aid is recommended for the most severe cases, with a battery whose size is easily noticed by the individual, enabling it to be handled, maintained and cleaned. In these cases, option can be made for a hearing aid with a remote control or with controls and battery partition easily located or regulated by remote control (10).
- Dental alteration and/or temporomandibular joint dysfunction (TM): these alterations can impair the adaptation of the hearing aid in relation to the acoustic gain, microphonia control, physical comfort and even the placement of the microchannel hearing aid or molds in the external acoustic meatus (24).
2. Audiological history: identification of the hearing complaint, time of hearing deprivation, life profile and the environments to which the individual is exposed every day, i.e., the acoustic variations in which he lives. This information enables to choose technology, acoustic programs and esthetical harmonization for a bigger period of daily use and benefits by using the hearing aid.
3. Hearing needs: specific daily situations that can be improved will enhance the individual's quality of life. The answers achieved in the COSITM - Client Oriented Scale of Improvement (Australian Hearing (25)) questionnaire enable the case-specific guidance and assistance, as well as to make the expectations with respect to the usage of the hearing aids more realistic, enhancing acceptance and the drive of the adaptation process.
4. Hearing aid selected for home test with chosen electroacoustic and structural specifications: home test is important to verify the individual's first response to the use of the hearing aid. In this period, it is essential to return regularly to the doctor for adjustments based on the individual's perception.
Part III - Verifying the hearing aid
Verification is intended to observe whether the characteristics designed in the hearing aid were achieved (1). In this process of verification, choice must be made for objective and subjective measures (7-9). The examinations performed in this service will be described:
1. Test of speech recognition in an open field:
This test compares the individual's hearing performance in conditions with and without the hearing aid (12). For the tests, a list of words (26) and/or sentences (27) in the Brazilian Portuguese is applied in accordance with the silence situation stages and the concurrent Speech-Noise-type noise (sign-noise relation: +10dB, 0dB or -10dB) in the contralateral acoustic box. In this test, the hearing performance is evaluated with the hearing aid in both ears and/or one ear at a time.
The test is performed inside an acoustically treated cabin, and the individual is positioned at a 60 cm-distance, at a 0º azimuth in relation to the acoustic box and at 120º azimuth to the contralateral acoustic box, with the head in horizontal line in relation to the sound source.
2. Amplified visible speech mapping (VSM)
VSM is a verification tool of the hearing dynamic field and the guidance to use the hearing aid that enables a bigger understanding of the benefits provided by amplification, more accurate adjustments and more individual's involvement in the process, as well as the guidance about possible restraints related to the case (28). This procedure uses the screen visualization of the amplification of real-life stimuli by the individual without requiring temporary deactivation of any specific algorithm, with an analysis of the hearing aid exactly in its in loco function.
The test is performed in a room with a controlled noise level, and the individual is positioned at a 60 cm-distance, at a 0º azimuth in relation to the acoustic box, with the head in horizontal line in relation to the sound source (acoustic box).
After equalizing the probe microphone by way of calibration, this tube is inserted into the individual's external acoustic meatus, reaching 27-30 mm deep. The hearing aid is then positioned in the individual's ear and switched on to perform the procedure.
The test is made with three levels of stimuli, smooth (45-55 dBNPS) kind of "cafeteria", medium (60-65 dBNPS) kind of spontaneous speech and ICRA-PB6-NTM , at least, strong intensity (85-95 dBNPS) kind of airplane noise. For the spontaneous speech stimulus, the list of words in Brazilian Portuguese (26) or the list of sentences is applied.
At the end of the test, it is verified if the stimuli are found inside the hearing dynamic field with the hearing aid.
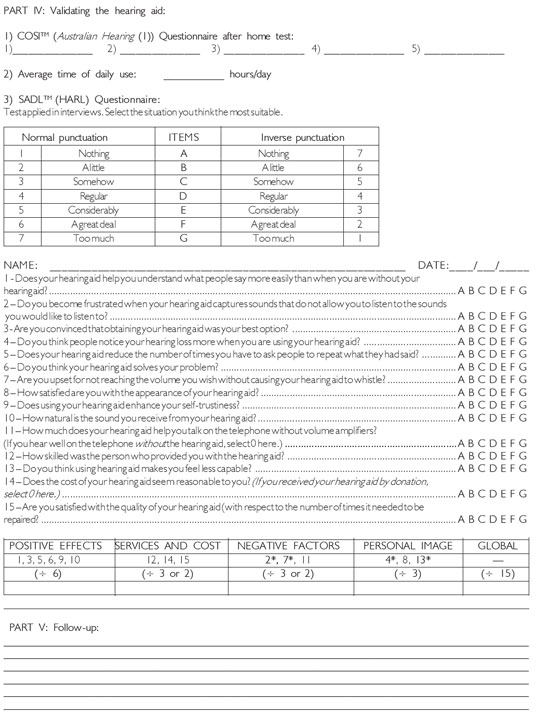
Part IV - Validating the hearing aid
The principle of validation is to measure the benefit and satisfaction provided by amplification, including individual's better quality of life, social relationship and emotional state (1). The procedures performed in this stage shall be described:
1. COSITM (Australian Hearing (25)) Questionnaire after home test: in this stage, after the hearing performed is measured by the objective methods, the items listed in the COSITM are analyzed and it is observed whether there was any difference with the hearing aid. The answers will help modify the programming of the device when required.
2. Average time of daily use: M measured by the informal approach or the objective analysis of the data registration built in the electroacoustic circuit of the digital hearing aid, it is observed the time of use and the characteristics of noise of the environment during the use. The time of use enables to evaluate whether the adaptation is effective, as well as the function of resources activated in the programming of the auditory loss (29).
3. The Satisfaction with Amplification in Daily Life - SADLTM (30) Questionnarie: it is considered that the use is directly related to the satisfaction and hearing performance provided by the use of amplification. The questionnaire SADLTM, applied one month after the adaptation of the hearing aid, has the purpose of evaluating the overall satisfaction or within four subscales: positive effects (items related to the acoustic and psychological benefit), services and cost, negative factors (approach about amplification of environmental noise, acoustic feedback and use of telephone) and personal image (items dealing with esthetical factors and the stigma associated with the utilization of the hearing aid). The bigger the punctuation achieved inside the subscale or in the global average the bigger the individual's satisfaction will be.
FINAL COMMENTARIESThe phonoaudiological hearing aid fitting protocol for adults and elderly shows that a great number of collected information provides a better orientation, adjustment to attain actual expectations and recommend hearing aids, thus allowing for the maximum hearing performance associated with the individual's satisfaction and benefit.
BIBLIOGRAPHICAL REFERENCES1. Matas CG, Iório MCM. Verificação e validação do processo de seleção e adaptação de próteses auditivas. In: Almeida K, Iório MCM. Próteses auditivas: fundamentos teóricos e aplicações clínicas. 2ª ed. São Paulo: Lovise; 2003, pp. 306-22.
2. Meister H, Walger M, Brehmer D, Wede U, Wedel H. The relationship between pre-fitting expectations and willingness to use hearing aids. Int J Audiol. 2008, 47(4):153-9.
3. Kochkin S. MarkeTrak V: "Why my hearing aids are in the drawer": The consumers' perspective. Hear J. 2000, 53(2):34-41.
4. Goggins S, Day J. Efficacy of recalling adult hearing aid users for reassessment after three years within a publicy-funded audiology service. Int J Audiol. 2009, 48:204-10.
5. Sinks BC, Duddy D. Hearing aid orientation and counseling. In: Valente M. Strategies for Selecting and Verifying Hearing Aid Fittings. 2ª ed. New York: Thieme Medical Publishers; 2002, pp. 345-68.
6. Citron III D. Counseling and orientation towards amplification. In: Valente M, Hosford-Dumh, Roeser RJ. Audiology Treatment. 2ª ed. New York: Thieme Medical Publishers; 2002, pp. 292-343.
7. Mueller G. Fitting test protocols are 2 more honored in the breach than the observance. Hear J. 2003, 56(10):112-24.
8. Brasil. Ministério da Saúde. Portaria Nº 587 de 7 de outubro de 2004, Anexo IV. 2004. Disponível em: portal.saude. gov.br/portal/sas/sapd/visualizar_texto. cfm?idtxt=22642
9. International Society of Audiology. Good practice guidance for adult hearing aid fittings and services - Background to the document and consultation. 2005. Disponível em: www.isa-audiology.org/ members/pdf/GPG-ADAF.pdf
10. Russo ICP, Almeida K, Freire KGM. Seleção e Adaptação da Prótese Auditiva para o Idoso. In: Almeida K, Iório MCM. Próteses auditivas: fundamentos teóricos e aplicações clínicas. 2ª ed. São Paulo: Lovise; 2003, pp. 385-410.
11. Cox RM. "Waiting for evidence-based practice for your fittings? It's here". Hear J. 2004, 57(8):10-7.
12. Mueller HG: Speech audiometry and hearing aid fittings: Going steady or casual acquaintances? Hear J. 2001, 54(10):19-29.
13. Mueller GH, Bentler RA, Wu YH. Prescribing maximum hearing aid output: differences among manufacturers found. Hear J. 2008, 61(3):30-6.
14. Ferrari GMS, Sanchez TG, Pedalini MEB. A eficácia do molde aberto para o controle do zumbido. Rev Bras Otorrinolaringol. 2007, 73(3):370-7.
15. Paulin F, Zeigelboim BS, Klagenberg KF, Rosa MRD. Achados vestibulares em usuários de aparelho de amplificação sonora individual. Rev CEFAC. 2009, 11(1):68-75.
16. Goebel J, Valente M, Valente M, Enrietto J, Layton KM, Wallace MS. Fitting Strategies for Patients with Conductive or Mixed Hearing Loss. In: Valente M. Strategies for Selecting and Verifying Hearing Aid Fittings. 2ª ed. New York: Thieme Medical Publishers; 2002, pp. 272-86.
17. Souza CD, Glasscock ME. Hearing Aids and Otosclerosis. In: Souza CD, Glasscock ME. Otosclerosis and Stapedectomy: diagnosis, management and complications. New York: Thieme Medical Publishers; 2004, pp. 69-72.
18. Arlinger S. Negative consequences of uncorrected hearing loss - a review. Int J Audiol. 2003, 2:17-20.
19. Pupo AC, Pirana S, Spinelli M, Lezirovitz K, Netto RCM, Macedo LS. Estudo de família brasileira portadora de deficiência auditiva sensorioneural não-sindrômica com herança mitocondrial. Rev Bras Otorrinolaringol. 2008, 74(5):786-9.
20. Meding B, Ringdahl A. Allergic Contact Dermatitis from the Earmolds of Hearing Aids. Ear and Hear. 1992, 13(2):122-4.
21. Maia CAS, Campos CAH. Diabetes Melittus como causa de perda auditiva. Rev Bras Otorrinolaringol. 2005, 71(2):209-14.
22. Mondelli MFCG, Lopes AC. Relação entre a Hipertensão Arterial e a Deficiência Auditiva. Arq Int Otorrinolaringol. 2009, 13(1):63-8.
23. Machado JAVP, Tôrres GM, Barcellos NA, Valle LT, Teixeira L, Fonseca MT. Incidência de Sintomas Otológicos em Pacientes Submetidos a Hemodiálise. Arq Int Otorrinolaringol. 2006, 10(1):62-6.
24. Hall CM. Clinical experience using a hearing aid for TMJ-related fitting problems. Hear Rev. 2004, 11(4):50-3.
25. Dillon H, James A, Ginis J. Client Oriented Scale of Improvement (COSI) and its relationship to several other measures of benefit and satisfaction provided by hearing aids. J Am Acad Audiol. 1997, 8(1):27-43.
26. Russo ICP, Lopes LQ, Bruntto-Borgianni LMB, Brasil LA. Logoaudiometria. In: Momenshon-Santos TM, Russo ICP. Prática da audiologia clínica. 5ª ed. São Paulo: Cortez; 2005, pp. 135-54.
27. Costa MJ, Iório MCM, Mangabeira-Albernaz PL. Desenvolvimento de um teste para avaliar a habilidade de reconhecer a fala no silêncio e no ruído. Pró-fono. 2000, 12(2):9-16.
28. Ross T, Smith KE. How to use live speech mapping as part of a hearing fitting and verification protocol. Hear R. 2005, 12(6):40-6.
29. Mueller HG. Data logging: It's popular, but how can this feature be used to help patients? Hear J. 2007, 60(10):19-26.
30. Cox RM, Alexander GC. Validation of the SADL questionnaire. Ear Hear. 2001, 222(2):151-60.
1 Master in Health Sciences from the Medical School of the University of Sao Paulo. Phonoaudiology at Otorhinolaryngology Foundation.
2 Doctor in Sciences from the Medical School of the University of Sao Paulo. Phonoaudiology at Otorhinolaryngology Foundation.
3 Progress in Cochlear Implant from the Clinical Hospital of the Medical School of the University of Sao Paulo.. Clinic Phonoaudiology.
4 Main Professor at the Medical School of the University of Sao Paulo.
Institution: Otorhinolaryngology Department of the Medical School of the University of Sao Paulo - Audiological Center at Otorhinolaryngology Foundation.
São Paulo / SP - Brazil. Mailing address: Juliana Harumi Iwahashi - Rua Teodoro Sampaio, 352 conj. 151 - Pinheiros - São Paulo / SP - Brazil - ZIP Code: 05406-000 -Telephone / Fax: (+55 11) 3062-9328 - Email: ju_iwahashi@uol.com.br
Article received on May 18, 2010. Article approved on July 18, 2010.