INTRODUCTIONMicrolaryngoscopy The suspension has been used for diagnostic purposes and therapy in various laryngeal disorders. Ideally, the visualization of the entire vocal fold, to the anterior commissural in order to avoid diagnostic errors, incomplete removal of lesions, inadvertent injury of the vocal cords (vocal folds), or even the abortion procedure. In most cases, the rigid laryngoscope of suspension allows adequate exposure of the larynx. However, some patients have difficulty in laryngeal exposure, one of the main problems in microsurgery of the larynx.
Several studies addressing preoperative clinical factors that predict the difficulty of endotracheal intubation for surgical procedures. These include the body mass index, modified Mallampati index, neck circumference, protrusion of the mandible, the test bite lip, the inter-incisor distance, the distance hiomentual, tireomentual the distance, the distance esternomentual the greater horizontal distance from the jaw, among others (1,2). Anaesthetists using the scale of Cormack and Lehane, to graduate the difficulty of endotracheal intubation, with a focus on visualization of the larynx, by raising the epiglottis by laryngoscope (1). However, these same parameters were evaluated just for the hiring of the laryngoscope, the attainment of microsurgery of the larynx. Moreover, there is no standard scale used by surgeons of the larynx.
This work aims to:
1) create a standard scale of difficulty leasing the laryngoscope during microsurgery of the larynx, with a focus on exposure of the vocal folds,
2) evaluate which clinical parameters predict difficult visualization of the larynx,
3) to verify the improved exposure of the vocal folds with the hanger of the laryngoscope.
METHODProspective study of patients undergoing microsurgery of the larynx in the period from July to December 2009 at the Department of Otorhinolaryngology, University Hospital of Curitiba, Federal University of Parana and Parana Institute of Otolaryngology.
This study was approved by the Ethics Committee of both institutions.
Regardless of the indication for surgery, all patients in this period, who agreed to participate in the survey were submitted to a protocol divided into preoperative and intraoperative evaluation.
Patients younger than 12 years were excluded from the study due to anatomical differences and the lack of reference values of the indices assessed. Also excluded were patients with rheumatic diseases, with osteoarthritis of the cervical spine and / or with extensive laryngeal lesions. These, because those changes made it difficult to correct classification of Cormack-Lehane scale and the scale proposed by the authors.
Patients were intubated with endotracheal tube (diameter 5.5 or 6.0 mm) under general anesthesia and muscle relaxant. After endotracheal intubation with the patient supine, without pillows under the head, neck or chest, with cervical flexion and extension of the head (position Boyce-Jackson) (3) (Figure 1), allocated to the laryngoscope Dan universal suspension (Figures 2 and 3). The universal laryngoscope Dan has only one size, 18 cm long, 2 cm in diameter in height and 1.5 cm in diameter in width. In cases of difficult laryngeal exposure was used compression of skin at the projection of the anterior commissure in the thyroid cartilage, on the outside of the neck. This, done by manual compression, performed by instrumentation, or a tape adhesive tape, compressing it, and fixed the edges of the head of the table.
Preoperative evaluation
Preoperatively, only two doctors are interspersed and collected the following data:
- epidemiological data: age, sex and indication for surgery;
- the anamnesis: snoring, rheumatologic disease, cervical changes and cervical trauma history;
- clinical variables: weight, height, missing teeth, neck circumference, modified Mallampati index, protrusion of the mandible (assessed by the test bite lip), neck flexion and extension, mouth opening (assessed by the inter-incisor gap) hiomentual distance in the neutral position (DHMn) and neck extension (DHM), distance tireomentual in neck extension (DTM), distance esternomentual in neck extension (DEM) and greater horizontal distance from the mandible (MDHM). We calculated BMI and the ratio of the distance hiomentual in neck extension / distance hiomentual neutral position.
The neck circumference was measured in centimeters at the time of the thyroid cartilage.
The modified Mallampati index was graded as follows: grade 1 = tonsils, pillars and soft palate visible; grade 2 = only uvula, pillars and upper pole of the tonsils visible, grade 3 = soft palate visible; grade 4 = only hard palate visible.
The test bite the upper lip was performed according to the following criteria: grade 1 = lower incisors bite the upper lip above the vermilion line, class 2 = lower incisors bite his lower lip below the vermilion line, class 3 = incisors can not bite the lower lip (2).
Flexion of the head was assessed asking the patient to hold the neck on the chest. Classified as normal when possible, otherwise as limited. Asking patients to extend the neck to evaluate the cervical extension.
The inter-incisor gap was measured with the mouth open to maximum, the tip of the lower incisor, in centimeters.
The neutral position was defined as the patient sat looking straight at the time of his eyes, his mouth closed. The position with the neck in extension was measured by asking the patient to extend the most of your neck.
The DHM, DTM and DEM were measured in centimeters, the prominent chin to the hyoid bone, thyroid cartilage prominence and top edge of the sternal notch, respectively (Figure 4).The MDHM was measured in centimeters in the mandibular angle prominence to the chin.
Intraoperative evaluation
During endotracheal intubation, the anesthesiologist evaluated the visibility larynx with the laryngoscope, as the scale of Cormack-Lehane: grade 1 = whole glottis is visible; class 2 = vocal cords partially visible or just the posterior commissure, class 3 = only the epiglottis is visible and grade 4 = epiglottis is visible (1).
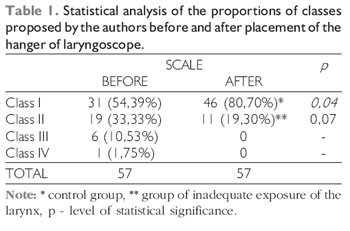
With the suspension laryngoscope at least two surgeons, different from that applied the procedure pre-operatively, assessed the laryngeal view. Classified according to the scale proposed by the authors (Table 1a). Before using the hanger and after placement of the hanger and, if necessary, use tape to tape and / or manual compression.
Reference Values
Limits were considered and evaluated statistically as predictors of difficult laryngeal exposure: BMI> 25, cervical circumference> 40 cm, the inter-incisor gap <4 cm, DHM <6.05 cm, DHM / DHMn <1.2 cm, DTM <7.15 cm, DEM <13.9 cm and MDHM <9 cm (4,5).
Define the classes proposed by the authors, after placing the hanger of the larynx, as follows: Class I = ideal exposure of the larynx, Class II = inadequate exposure and classes III and IV = difficult laryngeal exposure (Table 1a). The class I was considered as control group and compared with others.
Statistical Analysis
According to the nature of the data analyzed were judged appropriate statistical processing. Tests were applied: Student's t for the difference between the mean age and BMI between groups I and II, the scale proposed by the authors using the hanger laryngoscope, observing the normal distribution (Gaussian) of variables of difference in proportions before and after placement of the laryngoscope hanger for the whole group, chi-square or Fisher, when one of the cells with n <5 for the other variables between classes I and II proposed by the authors using the suspensor the laryngoscope. The level of significance was p <0.05.
RESULTSWe included 57 patients in the study, 30 female patients (52.63%) and 27 males (47.37%). The age ranged 14-66 years, mean 42 years.
The most prevalent indication for surgery was polyps, with 21 cases (36.84%), followed by nine cases of laryngeal papillomatosis (15.79%), 9 intra-chordal cysts (15.79%), 5 of vocal nodules (8.77%), four structural lesions Minin (7.02%), 4 Heinke edema (7.02%), 2 leukoplakia (3.51%), two post-intubation granulomas (3.51%,) and a traumatic ulcer (1.75%).
Patients were classified according to the scale proposed by the authors before and after placement of the hanger of laryngoscope. After placement of the hanger of laryngoscope, the majority of patients, 46 (80.70%), had exposure of the ideal vocal folds (class I) and 11 patients had inadequate exposure of the larynx (class II). These two groups were evaluated statistically. We did not get any patients with difficult laryngeal exposure (classes III and IV). With the hanger of a laryngoscope patient grade IV laryngeal improved its exposure to class II, four cases were in class III to class II, two developed grade III to I, 6 remained in class II and 13 class II obtain ideal exposure (class I) (Table 1).
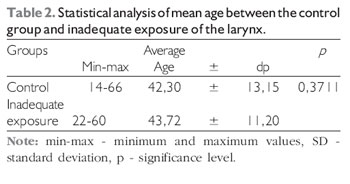
Comparing the control group with the group of inadequate exposure of the larynx, with regard to epidemiological factors: age (Table 2), gender (p = 0.59) and surgical indications, there was no statistical difference.
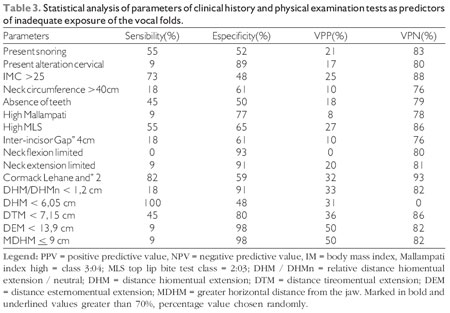
The parameters of clinical history and physical examination tests studied were evaluated as predictors of poor laryngeal exposure (Table 3).
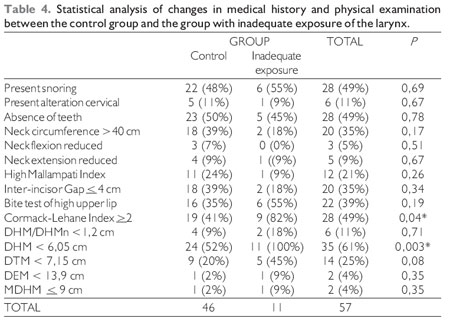
Parameters assessed in the interview, 28 had snoring and sixth cervical abnormalities (Table 4). Of these, four had a history of cervical trauma without fracture, 1COM torticollis and 1 with sporadic pain on lateral rotation of the neck.
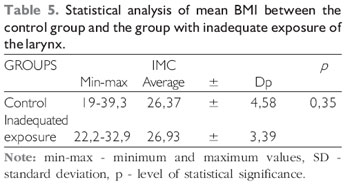
Of data collected during the physical examination, BMI in the total group ranged from 19 to 39,3; average 26.45 (Table 5).
One patient had undergone surgery for correction of micrognathia had MDHM 10 cm, showed optimum viewing of the larynx.
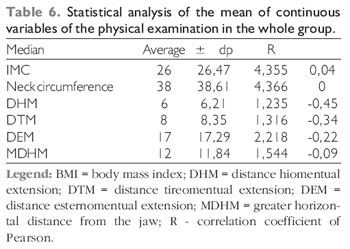
Continuous variables were analyzed for their mean, SD and r value (Table 6).
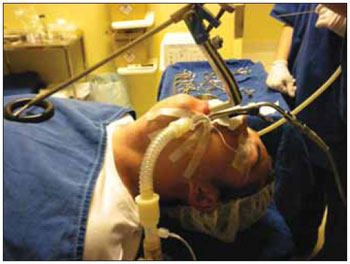
Figure 1. Position of the patient, and hanger suspension laryngoscope laryngoscope. - Patient ready to perform the microsurgery of the larynx, the Boyce-Jackson position, with the suspension laryngoscope and Dan universal hanger of laryngoscope allocated.

Figure 2. Laryngoscope universal suspension of Dan - Lateral view.

Figure 3. Laryngoscope universal suspension of Dan - Basal view.
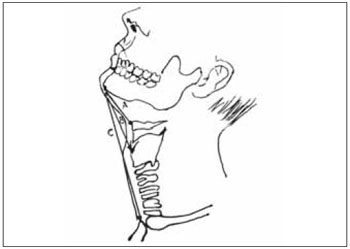
Figure 4. Some measurements performed preoperatively. - Patient with head extension. Distance hiomentual: the prominent chin to hyoid bone (A). Distance tireomentual: prominence of the chin prominence of thyroid cartilage (B). Distance esternomentual: the prominent chin to the top edge of the sternal notch (C).
Prior studies are not homogenous in terms of laryngeal view after the introduction of the suspension laryngoscope. Some studies divide patients into two groups: group of difficult laryngeal exposure, patients with limited exposure to the posterior third or less of the vocal folds, and the control group, the other patients (5,6,7). Not evaluating the cases of inadequate exposure of the larynx.
Other studies using a visual scale 10-10 (8), considered by the authors themselves, as cumbersome and subjective.
There is still work to consider the scale of Cormark-Lehane. Because the material used, the maneuvers and goals of the anesthetist in endotracheal intubation, differ from those of the laryngeal surgeon, using the same scale, or both, does not seem appropriate.
We can see the lack of a standard range of easy application that meets the needs of the laryngeal surgeon, plus the lack of standardization, making it difficult to compare studies.
Anesthesiologists consider the difficulty of endotracheal intubation classes 3:04 scale Cormack-Lehane. We propose to consider the class III and IV of the new scale (Table 1a) as the difficulty of hiring the laryngoscope and therefore of difficult laryngeal exposure. We suggest also consider other subdivisions: the class II, as inadequate exposure and class I as ideal exposure. Well, for the laryngeal surgeon, this subdivision may affect the completion and results of surgery.
The new scale proposed by the authors (Table 1a) seems to be appropriate and easy to use, for evaluation of laryngeal exposure during microsurgery of the larynx. Appropriate because it focuses on the vocal folds and considers the exposure of the anterior commissural. User-friendly by using only four classes intuitive.
Unlike previous studies, we have not had any cases of difficult laryngeal exposure itself. We found only 11 cases (19.30%) of inadequate exposure of the larynx. We stress that our study patients were candidates for difficult exposure. As an example, the average BMI was around 26, ie above the value considered predictive of difficulty of exposure (Table 5). Or, 20 patients had neck circumference above the cutoff value, 40 cm (Table 4). Question to racial factors, interfering with the referential values of the variables, and the role of different types of laryngoscopes, affecting the comparison between different studies (5,6). Perhaps a limitation of this study is the use of only one type of laryngoscope used infrequently, the laryngoscope Dan Used in this work to be routine and the preference of the authors.
As expected, the hanger of laryngoscope significant improvement in the exposure of the vocal folds (p = 0.04 for class I). Twenty patients (35%) improved exposure to its use (Table 1).
In this study, the laryngeal exposure score was significantly correlated with the Cormack-Lehane score used by anesthesiologists. This demonstrates that patients with difficult intubation are also inappropriate candidates for laryngeal exposure. A fact confirmed in other studies (5,6,8).
HSIUNG et al found sex as the most significant factor in predicting difficult laryngeal exposure (6). In this study, no differences according to sex. As for other epidemiologic factors examined, age and surgical indication. The two groups were age, surgical indication and sex distribution were similar (Table 2).
The evaluation of surgical indication, as a predictor of difficult laryngeal exposure was an innovation of this study.
Several parameters had a high sensitivity index: BMI> 25th, Cormarck-Lehane index > 2, DHM. High specificity: Mallampati index > 2, limited flexion of the neck, among others. Or, high NPV, as index-Lehane Cormarck > 2, DTM <7.15 cm, among others (Table 3). However, only reached statistical significance with the DHM (p = 0.003) and index-Lehane Cormarck > 2 (p = 0.04) (Table 4).
We searched the snoring, as an indicator of obstructive sleep apnea (OSA), since patients often have difficulty with SOAS intubation (8,9). However the presence of snoring was similar in the two groups.
PINAR et al (5) notorious that the measures of physical examination with the neck in extension were more reliable predictors than with the head in neutral position. Probably because they are closer to that used during the lease of the laryngoscope. Therefore, we evaluated only the measures in length.
Pinar et al associated with BMI, neck circumference and measures of DHM and TMD in length, with difficult laryngeal exposure (5). We evaluate all these parameters. However, only DHM <6.05 cm was statistical correlation with inadequate exposure (P = 0.003), with high sensitivity.
CONCLUSIONThe only parameters that showed significant correlation with inadequate exposure of the larynx were the distance hiomentual with head extension of less than 6.05 cm (p = 0.003) and index-Lehane Cormarck > 2 (p = 0.04).
The use of the hanger of laryngoscope improved laryngeal visualization significantly (p <0.04).
The range proposed by the authors seem to be appropriate and easy to use for exposure assessment during laryngeal microsurgery of the larynx. With the visualization of the vocal folds subclassified and standardized communication between otolaryngologists should be facilitated as well as future studies.
BIBLIOGRAPHICAL REFERENCES1. Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia. 1984, 39:1105-1111.
2. Khan ZH, Kashfi A, Ebrahimkhani E. A comparison of the upper lip bite test (a simple new technique) with modified Mallampati classification in predicting difficulty in endotracheal intubation: a prospective blinded study. Anesth Analg. 2003, 96:595-599.
3. Hochman II, Zeitels SM, Heaton JT. Analysis of the forces and position required for direct laryngoscopic exposure of the anterior vocal folds. Ann Otol Rhinol Laryngol. 1999, 108:715-724.
4. Merah NA, Wong DT, Ffoulkes-Crabbe DJ, Kushimo OT, Bode CO. Modified Mallampati test, thyromental distance and inter-incisor gap are the best predictors of difficult laryngoscopy in West Africans. Can J Anaesth. 2005, 52:291-296.
5. Pinar E, Calli C, Oncel S, Selek B, Tatar B. Preoperative clinical prediction of difficult laryngeal exposure in suspension laryngoscope. Eur Arch Otor. 2009, 266:699-703.
6. Hsiung MW, Pai L, Kang BH et al. Clinical predictors of difficult laryngeal exposure. Laryngoscope. 2004, 114:358-363.
7. Kawaida M, Fukuda H, Kohno N. Video-assisted rigid endoscopic laryngosurgery: Application to cases with difficult laryngeal exposure. J Voice. 2001, 15:305-312.
8. Hekiert AM, Mick R, Mirza N. Prediction of difficult laryngoscopy: does obesity play a role? Ann Otol Rhinol Laryngol. 2007, 116(11):799-804.
9. Mallampati SR, Gatt SP, Gugino LD et al. A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J. 1985, 32:429-434.
10. Hiremath AS, Hillman DR, James AL et al. Relationship between difficult tracheal intubation and obstructive sleep apnea. Br J Anaesth. 1998, 80:606-611.
1 Resident in the third year of the Department of Otorhinolaryngology, HC-UFPR.
2 Doctor. Medical Chief of the Laryngology of Otorhinolaryngology, HC-UFPR and IPO.
3 Academic Travel Medicine, UFPR.
4 Collaborating Professor, Department of Laryngology of the HC-UFPR.
5 Doctoral Course of Medicine, UFPR.
6 Head and Professor of Otolaryngology Department of the HC-UFPR.
Institution: Department of Otolaryngology, Hospital de Clinicas, Federal University of Parana and Parana Institute of Otolaryngology. Approved by the Ethics Committee of the two services. Curitiba / PR - Brazil. Mail Address: Annelyse Cristine Ballin - Rua Antonio Escorsin, 674, Don Carlo Condominium, house 31 - Curitiba / PR - Brazil - Zip code: 82015-000 - Telephone: (+55 41) 8406-8293 - E-mail: anneballin@uol. com.br
Article received in February 11, 2010. Article accepted in May 31, 2010.
Winning work in the Department of Otorhinolaryngology, HC-UFPR for best work done by residents in 2009.