INTRODUCTION The lagochilascariosis is an emerging zoonosis determined by the presence of helminth Lagochilascaris minor in human tissues. In the literature, is described five species of the genus,L. the only minor associated with human infections, which in adulthood affects approximately 50-20 mm in compliance with (1,2,3).
Wild animals are considered natural hosts are humans, dogs, cats and accidental hosts (2,4). CAMPOS et al. (1992) described the experimental life cycle of L. minor. These authors confirmed the hypothesis formulated by SMITH et al. (1983) that human infection is caused by ingestion of raw or undercooked meat containing larvae encysted in tissues of rodents, intermediate hosts (2). In the stomach the larvae hatch from the nodules and migrate through the esophagus to the upper digestive tract (2).
Lagochilascaris minor infection is rare, insidious, chronic condition, characterized by the appearance of festering abscesses located in the neck, mastoid, ear, nose and oropharynx.Occasionally, other structures such as the nasopharynx, brain, lungs, sinuses, Eustachian tube, dental and eye sockets, may be affected. Disease severity depends on the location of the lesion, the reproductive capacity of the parasite, even by the incursion of tissues and host immune response (1,2,3,6,7).
The diagnosis is based on identification of eggs, larvae and adult worms present in the secretions of the parasite in the lesions. Radiological examinations are useful in showing the location and extent of injuries, aiding in clinical management to be followed (3).
The following therapy with the use of Albendazole, Levamisole and Diethylcarbamazine in high doses. However, recurrences are common even after months of healing. Surgical removal of the larvae is a resource used to shorten the healing (2,7,10).
Worldwide Brazil ranks first in cases of human infection Lagochilascaris minor, mostly coming from the north, especially the state of Pará (7).
This paper introduces the presentation of a case, its relevance lies in the fact that arose in the rare case in the clinic of otolaryngology and other specialties. There were no records of attendance of such disease in recent decades, possibly by the rarity of its occurrence.
In this report the authors describe a case of otomastoiditis by L. minor in child, from the state of Mato Grosso, seen at Hospital das Clinicas, Federal University of Goiás, in Goiânia.
CASE REPORT SLQ patient, 10 years old, female student, a native of Barra Herons (MT), from rural areas of the city of South Australia (MT), came to the emergency department of Otorhinolaryngology, Hospital das Clinicas (HC), Federal University Goiás (UFG) in April 2004 with the following clinical features: severe otalgia, purulent otorrhea, hyperemia and retroauricular bulging right.
The guardian said that in the last two months the child presented with swelling, pain with purulent discharge in the right ear, looking for a health unit in your town, being seen by an ENT specialist who performed the drainage of the abscess by retroauricular incision with no improvement, evolved to purulent secretion through the hole.
In the clinical evaluation and oropharyngoscopy rinofaringoscopia earlier showed no change. Otoscopy left ear was normal, while the right ear had retroauricular edema, polyps in the external ear canal and fistula with drainage of pus. The tympanic membrane was intact (Figure 1).
Based on the clinical patient was hospitalized with a diagnosis of right otomastoiditis being requested laboratory tests, whose results were normal at the time. Began drug therapy with intravenous antibiotics.
The procedures for computed tomography of the temporal bones revealed opacification of mastoid cells with hyperdense material in the middle ear, already audiometry detected conductive hearing loss of mild right with hearing thresholds within normal limits on the left (Figure 2).
Three days after the initial consultation, the patient underwent a right mastoidectomy. Once the incision, we found the presence of spongy subcutaneous tissue and purulent discharge in the region of the mastoid and middle ear. In the early postoperative infection has evolved with persistent otorrhea and retroauricular fistula.
Histopathology revealed granulation tissue containing interspersed linfohistioplasmocitário marked infiltrate and foreign body granuloma comprising fragments of parasites with chitinous layer. Owing to the fragmentation of the parasite could not identify it precisely, in this material.
In the Laboratory of Biology, Biochemistry and Immunology of Helminths (LBBIH) Institute of Tropical Pathology and Public Health (IPTSP) of UFG, the definitive diagnosis was established by stool examination of the secretion of retroauricular fistula with identifying the direct examination on fresh, eggs of L. minor and later by stool examinations (Figure 3).
After the diagnosis was given specific therapy with levamisole (150 mg / day) ivermectin (300 mg / kg / week) and later, albendazole (400 mg / day) with marked improvement otology. The patient was discharged with the same prescription for 40 days with a scheduled return later to the otorhinolaryngology from hospital after 90 days.
Three months after surgery the patient returns to the clinic, where he observed the formation of a discrete nodule adjacent to the previous injury, which was spontaneous elimination of a small live worm, according to a report of the patient's father. After removal, surgical histopathology revealed fragments of tissue with chronic granulomatous inflammatory reaction, containing interspersed cuts Lagochilascaris suggestive of parasite. Were prescribed two courses of albendazole at intervals of 15 days alternating with a weekly administration of ivermectin. The patient was advised to return to the clinic after six months for follow up treatment. After this period, he returned with no signs of otorrhea or ear infection right, being carried out further examination hearing whose outcome had to be within normal limits in both ears (Figure 4).
The patient was discharged, returning to his home city, and continued follow up with teams of infectious diseases and parasitology IPTSP HC-UFG.

Figure 1. Retroauricular fistula right. Seroporulent secretion drainage. SLQ patient resident of the rural area of South Australia (MT). HC-UFG 2004.
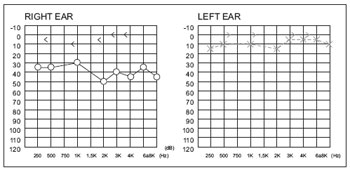
Figure 2. Audiometry. Conductive hearing loss of mild right with hearing thresholds within normal limits on the left. HC-UFG 2004.
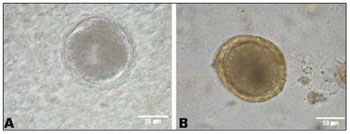
Figure 3. Lagochilascaris minor eggs in seropurulent secretion retroauricular fistula (A) and stool examinations (B) of patient SLQ resident of the rural area of South Australia (MT). IP TSP-UFG 2004.
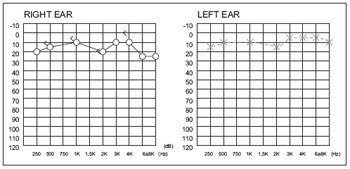
Figure 4. Audiometry. Normal hearing thresholds in both ears. HC-UFG 2005.
The interest in describing this case is evidenced in the rarity of its occurrence, as well as the conduct and outcome of it.
The diagnosis is based on identification of eggs, larvae and adult worms present in the lesions where surgical cleaning may help in healing. In this case the patient had a festering abscess in the mastoid region, during the surgical removal of the same, material was removed for biopsy showing a histological results suggestive of infection by L. minor confirmed later by stool examination of the secretion and faeces of patients (3,7,9,10).
Generally otological surgeries require some care to preserve the hearing of the individual. The patient's laboratory tests showed no changes are not supporting the diagnosis. However, tests such as computed tomography of the temporal bone and auditory helped in planning and surgical approach, as recommended by some studies (3,9).
The ingestion of game meat (armadillo and paca) was mentioned by the patient lying in the literature that the disease is acquired through ingestion of larvae encysted in the subcutaneous tissue, muscle and viscera of wild animals (1,3,4).
Whereas the process of recurrent disease, we used the prescription of albendazole and ivermectin for long time monitoring functions with renal, hepatic, hematopoietic and endocrine pancreatic throughout treatment. Measures such as maintenance medication and regular monitoring at the clinic until clinical improvement of symptoms were followed, as suggested by some authors (3,7,8,10). Disregard the recurrent process and neglect the maintenance and monitoring of the case may aggravate the same (9).
Throughout the treatment the patient was monitored by teams of otolaryngology, infectious diseases and parasitology of the institution.
FINAL COMMENTSThe joint treatment between the teams of otolaryngology, infectious diseases and parasitology as well as participation and cooperation of the patient and family coping with disease, appearing at all returns, closely following the prescription, confirmed for the successful treatment, whereas the same reside in another state.
The clinical significance remains to be careful in considering the differential diagnosis of this disease on individuals residing in rural areas. This serious parasitic disease can affect various structures of the body, severely compromising the health of the patient with serious complications that may lead to death.
BIBLIOGRAPHICAL REFERENCES1. Barbosa AP, Campos DMB, Semerene AR, Teixeira AR, Santana JM. Lagochilascaris minor third-stage larvae secrete metalloproteases whit specificity for fibrinogen and native collagen. Microbes Infect. 2006, 8:2725-32.
2. Campos DMB, Freire Filha LG, Vieira MA, Paçô JM, Maia MA. Experimental life cycle of Lagochilascaris minor Leiper, 1909. Rev Inst Med Trop São Paulo. 1992, 34:277-87.
3. Palheta-Neto FX, Leão RNQ, Neto HF, Tomita S, Lima MAMT, Pezzin-Palheta AC. Contribuição ao estudo da lagoquilascaríase humana. Rev Bras Otorrinolaringol. 2002, 68:101-05.
4. Barbosa CAL, Barbosa AP, Campos DM.Gato doméstico (Felis catus domesticus) como possível reservatório de Lagochilascaris minor Leiper (1909). Rev Pat Trop. 2005, 34:211-53.
5. Smith JL, Bowman DD, Little MD. Life cycle and development of Lagochilascaris sprenti (Nematoda: ascarididae) from opossums (Marsupialia: didelphidae) in Louisiana. J Parasitol. 1983, 69:736-45.
6. Semerene AR, Lino Junior RS, Oliveira JA, Magalhães AV, Stefani MM, Barbosa AP, Campos DMB. Experimental lagochilascariosis: histopathological study of inflammatory response to larval migration in the murine model. Inst. Oswaldo Cruz. 2004, 99:393-8.
7. Vieira MA, Oliveira JA, Ferreira LS, Oliveira V, Barbosa CAL. Relato de caso de Lagochilascariose humana procedente do Estado do Pará, Brasil. Rev Soc Bras Med Trop. 2000, 33:87-90.
8. Rocha MPC, Fraiha NH, Barreto NACP. Infecção de ouvido médio e mastóide por Lagochilascaris minor Leiper, 1909 (Nematoda, Ascaridiae). Relato de um caso do Sul do Estado do Pará, Amazônia, Brasil. Hiléia Médica. 1984, 6:3-14.
9. Baracat DA, Freire EL, Aquino JL. Oto-mastoidite crônica por Lagochilascaris minor com comprometimento da região temporo-parieto-occipital. Rev Univers Fed Mato Grosso. 1984, 2:9-14.
10. Monteiro AV, Zapotoski SMK,Torres DMAGV, Berenchtein MA, Pinto PLS. Infecção por Lagochilascaris minor Leiper 1909, no Vale do Ribeira, estado de São Paulo, Brasil (Relato de Caso). Rev Inst Adolfo Lutz. 2004, 63:269-72.
1 PhD. Responsible for Audiology Service of ENT Clinic of HC / UFG.
2 PhD in Molecular Biology. Associate Professor of Parasitology, Institute of Tropical Pathology and Public Health - UFG.
3 Master in Otorhinolaryngology. Substitute Professor of Clinical Otorhinolaryngology, Faculty of Medicine - UFG.
4 Expert in Otorhinolaryngology. Assistant Professor of Clinical Otorhinolaryngology, Faculty of Medicine - UFG.
5 Physician. MSc in Tropical Medicine Area of Concentration in Parasitology. Institute of Tropical Pathology and Public Health - UFG.
6 Resident in Otorhinolaryngology, Hospital das Clinicas - UFG.
7 PhD in Nursing. Professor, School of Nursing - UFG.
8 PhD in Parasitology. Professor of the Institute of Tropical Pathology and Public Health - UFG.
Institution: Hospital das Clinicas (HC) and Institute of Tropical Pathology and Public Health (IPTSP), Federal University of Goiás (UFG). Goiânia / GO - Brazil. Mail Address: Valerian de Castro Guimarães - Hospital das Clinicas, Federal University of Goiás - First Avenue, s / n - Setor Leste Universitário - Goiânia / GO - Brazil - Zip code: 74605-020 - E-mail: valeriana.guimaraes@gmail.com
Article received on May 2, 2009. Article accepted on June 21, 2009.