|
380 |
|
| Year: 2006 Vol. 10 Num. 3 - Jul/Set - (2º)
|
|
 |
| Section:
Original Article
|
|
|
|
|
| The Prevalence of Noise Induced Hearing Loss Among Textile Industry Workers |
|
| Author(s): |
| Adriano Ulisses Caldart1, Cíntia Felício Adriano1, Igor Terruel1, Rafael Ferri Martins1, Arnoni Ulisses Caldart2, Marcos Mocellin3
|
|
|
| Key words: |
| Hearing loss. Hoise-induced; noise. Occupational; noise control. |
|
|
 |
| Abstract: |
Introduction: In the Textile industry the work of the machines produce noise that can cause irreversible damage to workers hearing. Objective: The purpose of this research is to determine the prevalence of NIHL in workers of a textile industry in Brusque - SC, to verify its intensity, characterize the main hearing symptoms, observe the age groups most affected, indentify the riskiest sector and correlate with the time of exposure to the noise. Method: A transversal study of 184 workers divided proportionally in each sector of work, evaluated through interviews, otoscopic exam. and occupational audiometry. Result: The prevalence of NIHL was 28.3%, with predominance of hearing loss of 1st degree (46.2%), according to Meluzzi's classification. The most frequent symptoms were hipoacusis (30.8%), difficulty of understanding the words (25.0%), tinnitus (9.6%), auricular plenitude (5.8%), dizziness (3.8%) and hear pain (3.8%). The work sector with the highest rate of NIHL was industrial engineering with 44.4%, followed by spinning with 38.9% and weaving with 38.8%, PPD (processing, printing and dryer) with 23.8% and administration with 3.8%. The age group most affected was from 50 to 64 years old. The workers who had been working for more than 20 years were also the most affected (42.9%). Conclusion: The occurrence of NIHL was significant in 1st degree, associated to hipoacusis. The riskiest sectors in the industry are engineering, spinning and weaving. There was an increase of the cases because of the age and time of exposure.
|
|
|
INTRODUCTION
In industries in general and especially in textile one, machinery produces such noise that when intensified can cause damages to worker´s hearing. Lon-term noise exposure can cause hearing loss.
Hearing damages caused by noise-induced hearing loss (NIHL) arises from alterations on internal structure of cochlea that cause irreversible damages and symptoms such as hypoacusis, tinnitus, auricular plenitude and otalgia (ear pain). Levels of noise higher than 85 dBNA for 8 daily hours for a long period are enough to cause cochlea damage (1).
NHIR diagnosis is performed by history of exposure in noise environment, ENT exam focused on otoscopy and audiometric exam. Hearing loss should have been developed in a gradual way in a period from around 6 to 10 year of continuous exposure at high levels of noise. Otoscopy and physical exam are in normal condition. Audiometric exam always reveals sensorineural and irreversible hearing loss and symmetric in general, in frequencies from 2000 to 4000 Hz (2).
Apart from knowledge of diagnosis and prevention programs used in industries, this pathology still represents a serious problem of occupational health, especially in textile industries. The studies by GITAU et al. (3), NGUYEN et al. (4), BERLACHEW & BERHANE (5), OSIBOGUN et. al. (6) and SHAKHATREH et al. (7) showed a high prevalence of NIHL in workers from textile industry. With the high number of such industry in Brazil, the number of people exposed to noise has been expressively increasing. Therefore, it is important monitoring worker´s hearing, early diagnosing and preventing NIHL through a program of hearing conservation.
The target of this study is to determine the prevalence of noise-induced hearing loss in workers from a textile industry in Brusque (SC), to verify pathology intensity, to characterize the main audiological symptoms, to verify the age of higher prevalence, to identify industry sector of higher risk and to relate cases with period of noise exposure.
METHOD
This transversal study was done from June to November in 2004. The industry employed 582 employees divided in weaving, spinning, industrial engineering, expedition, PPD (processing, printing and dryer) and administration departments, with levels of noise from 88,6 to 103 dB, 86 to 97 dB, 80 to 94 dB, 65 to 70 dB, 76 to 92 dB and from 65 to 74,4 dB, respectively. Such measures were performed during working time using a decibel meter Simpson - 886.
As NIHL needs at least 5 years to develop, employees working less than this period were excluded from tests. 343 employees remained and from those 184 were selected to raise a sample (error of 5% and confidence grade of 95%). They were divided proportionally in each sector: weaving (67), spinning (18), industrial engineering (18), expedition (8), PPD (42) and administration (31).
All workers were evaluated through a selection protocol composed by interview, otoscopic exam and occupational audiometry.
Workers were identified by their names, ages, genders, functions and noise exposure period during interview. It was also performed a hearing selection where questions on otological symptoms such as hypoacusis, tinnitus, speech understanding difficulty, dizziness, auricular plenitude, otalgia and otorrhea were asked. Questions on systemic diseases such as disorders of air pathways, DM SAH, syphilis, measles, mumps, thyreoid diseases, renal disorders and antecedents with previous otological problems, previous surgery, family history of non-occupational noise exposure were also asked.
After interview, it was performed otoscopy with a portable battery-rum gadget in order to evaluate external hearing canal and tympanic membrane.
And then, it was performed tonal audiometry and analysis of audiometric curves after a hearing rest of 14 hours at least (1). It was used an audiometer Interacoustics - AC 40 with yearly certificate calibration. Interpretations of tonal audiometry were classified according to DAVID and SILVERMANN´s criteria (8), and then audiometric curves suggesting NIHL were classified according to SANTINHO and COUTO (9). Lastly, audiometries suggesting NIHL were classified in intensity, according to Merluzzi´s classification (10).
Data were recorded and analyzed through a data base named Epi Info 2000, developed to epidemiological purposes.
The individuals signed a free and clear consent and approval term and the protocol was previously approved by Comitê de Ética em Pesquisa da Universidade do Paraná (Ethics Committee in Research).
RESULT
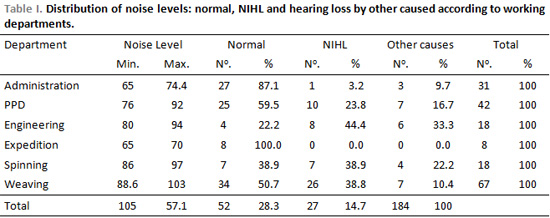
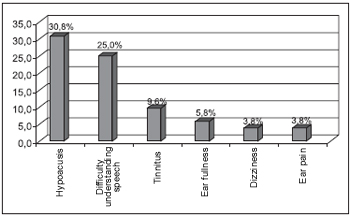
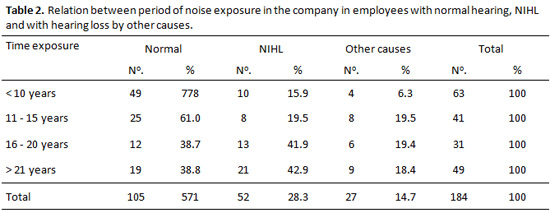
Sample was composed of 184 workers. 153 men and 31 women, aging from 18 to 64 year, working 8 hours a day, six days a week. Regarding hearing loss, 105 of them (57.1%) presented normal condition, 52 (28.3%) presented audiometric curves compatible with NIHL and 27 (44.7%) presented hearing loss by other reasons. Prevalence of intensity grades of NIHL, according to Merluzzi (10), can be seen in Picture 1. Table 1 shows noise level, percentage and number of workers with normal hearing, with NIHL and with hearing loss by other reasons regarding industrial sector. In relation to age, higher prevalence of NIHL was observed in the group of older worker, aging from 50 to 64 years. More frequent symptoms can be seen in Picture 2. Table 2 shows the relation of noise exposure period in the company with normal worker, with NIHL and hearing loss by other reasons. An increase on NIHL cases was verified as exposure period increased.
DISCUSSION
During researching, it was found high levels of noise in textile industry, raging from 65 dB to 103 dB. The noisiest sections were weaving, spinning and industrial engineering. COSTA (11), BELACHEW & BERHANE (5) and GITAU et al. (3) also refer textile industry as one of the noisiest ones, especially in weaving and spinning sections, what explains the prevalence of NIHL in such departments. The risk of developing NIHL lies on duration and level of noise at which worker is exposed, even wearing individual ear protectors, as this device reduces intensity of environment noise only in 10 to 15 dBNA (1).
Prevalence found in NIHL in worker was of 28.3%. BELACHEW & BERHANE (5), GITAU et al. (3), SHAKHATREH et al. (7), OSIBOGUN et al. (6) found prevalence of 34.0%, 32.5%, 30,0% and 79.8% respectively. MIRANDA et al (12) observed a prevalence of 23.4% lesser than the one found in this study. This prevalence of NIHL lesser than the others from the revised literature can be explained by the fact that in the industry where the study was done, preventive procedures have been performed for around 10 years, using ear protectors and performing audiometry tests on workers in noisy environment.
In relation to NIHL distribution through different departments of the company, the industrial engineering (44.4%), spinning (38.9%) and weaving (38.8%) had similar results. Although industrial engineering presented a percentage of around 5% higher than the other departments, this number was not expressive among industrial engineering, spinning and weaving departments, considering that error rate in sample process was 5%. BELACHEW & BERHANE (5) and GITAU et al. (3) pointed weaving with superiority (71.7% and 60.0% respectively), followed by spinning (35.2% and 37.7% respectively) as departments with higher prevalence of NIHL. These two departments were among the noisiest ones. These differences can be caused by factors referred by KWITKO (13), which are presence of variables such as age, gender, previous hearing pathology, associated diseases, audiometer calibration, technical problems on the booth and subjectivity of audiometric test.
The higher prevalence of NIHL cases was grade I according to Merluzzi (10) (45.1%) as well as to MIRANDA et al. (12) and SILVA et al (14), who observed with 20.6% and 25.6% respectively.
It was also possible to demonstrate that NIHL cases increased as working period in the company increased and that employees working for more than 20 years (i.e. 20 years of noise exposure) were the most affected ones with a rate of 42.9%. This reinforces that hearing consequences depend on intensity and period of noise exposure, according to COSTA (11) and BELACHEW & BERHANE (5).
Aging was also a factor that expressively increased the cases of NIHL, employees over 50 years were the most affected ones (46.2%). GITAU et al. (3), BELACHEW & BERHANE (5) and SILVA et al. (14) showed this relation.
Among hearing symptoms, hypoacusis was the most frequent one (30.8%), followed by speech understanding difficulty, tinnitus, auricular plenitude, dizziness and otalgia. ARAÚJO (2), by frequency order, found: tinnitus, speech understanding difficulty, dizziness, hypoacusis, otorrhea and sensation of auricular plenitude. OLIVEIRA et al. (15) observed that tinnitus was the most frequent symptom.
It was noticed that NIHL, grade I by Merluzzi (10), occurred despite preventive procedures had been taken along the years. This confirm the need of a effective follow-up, by the companies, with Hearing Conservation Programs, focusing employees and worker´s awareness regarding the importance of a regular use of hearing protectors.
CONCLUSION
One might conclude that prevalence of NIHL in industry was 28.3%, and most of cases was established as grade l, in 46.2% of affected workers, followed by grade 2 in 42.3%, grade 3 in 5.8%, grade 4 in 3,8% and grade 5 in 1.9%. In workers with NIHL, hypoacusis was the most frequent symptom (30.8%), followed by speech understanding difficulty in 25%, tinnitus in 9.6%, auricular plenitude in 5.8%, dizziness and otalgia in 3.8%. Employees aging from 50 to 64 years were the most affected ones. The risky departments were industrial engineering, spinning and weaving. There was an increase of NIHL as period of noise exposure increased, especially after 21 years of exposure.
REFERENCES
1. Nudelmann AA, Costa EA, Feligman J, Ibáñez RN. Perda auditiva induzida pelo ruído. Rio de Janeiro: Revinter; 2001.
2. Araújo SA. Perda auditiva induzida pelo ruído em trabalhadores de metalúrgica. Rev Bras Otorrinol, 2002, 68:47-52.
3. Gitau JM, Mwikali JM, Bett KW, Njau ZG. Noise induced hearing loss among textile industry workers in Eldoret, Kenya. Disponível em: www.medlib.iupui.edu/moi/gitaucobesiv.htm. Acessado em 16 Jun 2004.
4. Nguyen Al, Nguyen TL, Van TL, Hoang MH, Nguyen S, Jonia H, et al. Noise levels and hearing ability of workers in a textile factory in Vietnam. Ind. Health, 1998; 36:61-5.
5. Belachew A, Berhane Y. Noise-induced hearing loss among textile workers. Ethiop J Health Dev, 1999, 13:69-75.
6. Osibogun A, Igweze IA, Adeniran LO. Noise-induced hearing loss among textile workers in lagos metropolis. Niger Postgrad Med J 2000, 7:104-111.
7. Shakhatreh FM, Abdul-baqi KJ, Turk MM. Hearing loss in a textile factory. Saudi Med J 2000, 21:58-60.
8. Davis H, Silverman, SR. Hearing e deafness. 3rd ed. New York: Holt, Renenhart & Winston; 1970.
9. Santinho E, Couto HA. Audiometrias ocupacionais: guia prático. Belo Horizonte: Ergo; 1995.
10. Merluzzi F. Metodologia di esecuzione del controllo dell'udito dei lavoratori esposti a rumore. Nuovo Arch Ital Otol, 1979, 7:695-712.
11. Costa VHC. O ruído e suas interferências na saúde do trabalhador. Rev SOBRAC, 1994, 13:912-26.
12. Miranda CR, Dias CR, Pena YPGL, Nobre LCC, Aquino R. Surdez ocupacional em trabalhadores industriais da região metropolitana de Salvador, Bahia. Rev Bras Otorrinol, 1998, 64:109-114.
13. Kwitko A. Avaliação epidemiológica dos dados audiométricos ocupacionais. Rev ACTA AWHO, 1998, 17:193-202.
14. Silva LF, Santos SA, Shoraiski NY, Silva JS, Priorte SV, Koiski SM, et al. Estudo da prevalência da perda auditiva induzida por ruído em trabalhadores de uma indústria gráfica. Distúrbios da Comunicação, 1998;10:45-58.
15. Oliveira TMT. Implantação de um programa de conservação auditiva de uma indústria de bebidas. Rev Bras Saud Ocup, 2002;24:31-6.
1. Graduation Student (Resident Doctor in the third year of Otorhinolaryngology - UFPR)
2. Master student (ENT doctor - Master in Surgical Clinic by FURB/UFPR)
3. Doctorate (Titular Professor of ENT at UFPR. Head of ENT Service at Hospital das Clínicas da Faculdade de Medicina da Universidade Federal do Paraná)
Hospital de Clínicas da Universidade Federal do Paraná
Address: Rua General Carneiro, 181, 6o. andar - Anexo B, Bairro Centro, CEP 80060-900, Curitiba - PR
This article was submitted to SGP - Sistema de Gestão de Publicações (Publication Management System) from RAIO on July 13, 2006 and was approved on August 02, 2006 01:02:18.
|
|
 |
|
|