 |
530 |
|
| Year: 2008 Vol. 12 Num. 2 - Abr/Jun - (21º)
|
|
 |
|
|
| Labyrinthitis Ossificans. Report of One Case and Literature Review |
|
| Author(s): |
| Leandro Ricardo Mattiola1, Mark Makowiecky2, Carlos Eduardo Guimarães de Salles2, Marcela Pozzi Cardoso3, Samir Cahali4
|
|
|
| Key words: |
| labirinthitis, cochlea, hearing loss, osteogenesis |
|
|
 |
| Abstract: |
Introduction: Labyrinthitis ossificans is a pathology characterized by sensorioneural hearing loss; secondary to infectious process, which produces irreversible injury to inner ear. Objective: To report a labyrinthitis ossificans case and review the literature. Case Report: A seven-year-old male patient, with profound hearing loss in tonal audiometry; no response from brainstem audiometry and compatible CT findings. Conclusion: Labyrinthitis ossificans results ossification on the inner ear structures. Pacient presents profound irreversible hearing loss, followed or not by disequilibrium, that can have important implication on educational socio-development. Diagnosis is important for cochlear implantation cases of the selected cases.
|
|
|
INTRODUCTION
Ossification of membranous labyrinth or labyrinthitis ossificans (LO) is usually a sequela of a previous infection, especially suppurative labyrinthitis(1). It can develop through three ways of infection dissemination, such as hematogenic, meningogenic or tympanogenic way. LO is the final result of suppurative labyrinthitis regardless the origin of the infection(2). Other non-common causes account for tumors, advanced otosclerosis, breaking of temporal bone and hemorrhage of the inner ear(3). LO results profound hearing loss and also due to ossification process it can prevent cochlear implant (CI) (4,5). Computed Tomography (CT) has been of a great help to diagnose LO(6) and besides to evaluate the possibility of CI(7).
CASE REPORT
A 7-year-old male patient complained of hearing loss to the left for sixteen months. It was initially noticed by the mother and of slow progressive development. Patient only presented an incidence of acute medium otitis one month before, which improved after treatment, but no other previous history of otological infection. He did not present either learning difficulties, family history of hearing loss, gestational infection or other dysfunctions.
It could be observed tympanic membrane in normal condition by bilateral otoscopy; right lateral Weber's test and tonal audiometry with normal threshold to the right and profound hearing loss to the left. Auditory brainstem responses (ABR) presented normal condition to the right and no response to the left at 105 dB. CT of temporal bones revealed labyrinth ossification to the left.
DISCUSSION
Labyrinth injury resulting in profound hearing loss with cochlear ossification or LO can occur after any otological damage(8), and it is usually a sequela of infections. They can reach inner ear through blood flow (hematogenic), through middle ear (tympanogenic) or through meninges (meningogenic) (1,9). We believe that the LO pathology of the reported case was arose from tympanic labyrinthitis, however, there are no documented events of previous otological infection to hypoacusis. Tympanic labyrinthitis is the most common cause of LO(6). The route by which infection of the middle ear reaches the inner one was studied by several authors. These studies recognized the window of the cochlea as the main way for infection dissemination to the inner ear however, dissemination may also occur by the window of the vestibule or both windows. Paparella et al(10) described a high incidence of histopathological alterations in the inner ear, which are secondary to middle otitis. Such alterations were more frequently observed in the tympanic scale, what confirms that the window of the cochlea would be the main route for dissemination. Though ossification is thicker and more extensive in cases of meningogenic meningitis during childhood(11). In such cases, infection reaches inner ear through subarachnoid space, cochlear aqueduct and through inner acoustic meatus(1,6,12). Ossification usually occurs in bilateral way on these patients, and can be found 3-4 months after bacterial meningitis condition. Our patient did not present meningitis history and ossification developed unilaterally. Regarding hematogenic labyrinthitis, intrauterus infection is its main cause combined with German measles or mumps pathogens. Hematogenic labyrinthitis occurring from a hidden or distant focus is a rare(6). Traumas, comprising surgical one, are known pathogenesis, though their mechanisms are still indefinite. Regardless etiology, LO pathogenesis involves an acute initial stage, with the presence of bacteria and leucocytes often in the perilymphatic spaces. Then it follows a stage characterized by proliferation of fibroblasts and fibrosis which caused ossification. Fibroblasts are supposed to be the source for development of ligament substances and for the fibers of osteoid matrix(13). Hypoacusis is slowly progressive and a deep neurossensorial dysacusis is what usually ocurrs. This development was observed in the reported case. Patient can also experience dizziness at any degree either during acute infectious condition or during disease development(2). LO finding in the radiological evaluation is clinically important, because it justifies hypoacusis finding in the auditory exam, as well as occasional balance dysfunction of the involved side. CT may present sclerosis, irregularities or obliteration of the cochlea; semicircular vestibule or canals with different involvement degrees. Tomographic study of the disease extension may help to identify which patient will be benefited by CI(7). Ossification might make electrode implantation difficult. In the beginning, even a discreet LO was not considered to apparatus for multichannel cochlear implant(14). Nowadays there is a range of options. Moderate ossification of the basal turn can be conventionally perorated via facial recess approach. In more severe cases, the electrode can be partially inserted(15). There is no recommendation for cochlear implant in our case because contralateral hearing is in normal condition.
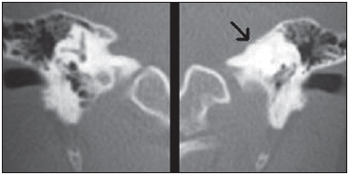 Picture 1 - Labyrinthitis ossificans to the left (arrow) and normal labyrinth structures to the right. 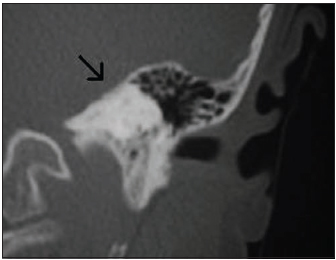 Picture 2 - Axail CT of temporal bone in coronal cut showing Labyrinthitis ossificans to the left (arrow)
FINAL CONSIDERATIONS
Inflammation on otic capsule of non- or infectious etiology is the beginning of a destruction process of the membranous labyrinth that reaches the ossification of inner ear structures. Also known as Labyrinthitis ossificans, it leads patients to experience irreversible profound hypoacusis, followed or not by unbalancing, what can involve socio-educational development. Diagnosis is favored by imaging exams, which are also important when recommending CI.
REFERENCES
1. Neely JG. Complications of temporal bone infection. In: Cummings CW et al: Otolaringology - Head and Neck Surgery. St Louis: Mosby Year Book; 1993, pp. 2840-2864.
2. Hoffman RA, Brookler KH, Bergeron RT. Radiologic diagnosis of Labyrinthitis Ossificans. Ann. Otol. 1979, 88:253-7.
3. Suga F, Lindsay JR. Labyrinthitis ossificans. Ann Otol Rhinol Laryngol. 1977, 86:17-29.
4. Balkany T, Gantz B, Nadol JB Jr. Multichannel cochlear implants in partially ossified cochleas. Ann Otol Rhinol Laryngol. 1988, 97(suppl 135):3-7.
5. Gantz BJ, McCabe BF, Tyler RS. Use of multichannel cochlear implants in obstructed and obliterated cochleas. Otolaryngol Head Neck Surg. 1988, 98:72-91.
6. Swartz JD, Mandell DM, Faerber EN, et al. Labyrinthine ossification: Etiologies and CT findings. Radiology. 1985, 157(2):395-8.
7. Weissman JL, Kamerer DB. Labyrinthitis Ossificans. Am J Otolaryngol. 1993, 14(5):363-5.
8. Hinojosa R, Redleaf MI, Green JD Jr, Blough RR. Spiral Ganglion Cell Survival in labyrinthitis ossificans: Computerized image analysis. Ann Otol Rhinol Laryngol Suppl. 1995, 166:51-4.
9. de Souza C, Paparella MM, Schacern P, et al. Pathology of Labyrinthine Ossification. J Laryngol Otol. 1991, 105(8):621-24.
10. Paparella MM, Oda M, Hiraide F, et al. Pathology of sensorineural hearing loss in otitis media. 1972, 81:632-47.
11. Green JD Jr, Marion MS, Hinojosa R. Labyrinthitis ossificans: Histopathologic consideration for cochlear implantation. Otolaryngol Head Neck Surg. 1991, 104:320-6.
12. Tinling SP, Brodie HA, Nabili V. Location and timing of initial osteoid deposition in postmeningitic labyrinthitis ossificans determined by multiple fluorecent labels. Laryngoscope. 2004, 114:675-80.
13. Tinling SP, Nabili V, Brodie HA. Fine Structure Histopatology of Labyrinthitis Ossificans in The Gerbil Model. Ann Otol Rhinol Laryngol. 2005, 114:161-6.
14. Westerlaan HE, Meiners LC, Penning L. Labyrinthitis ossificans associated with sensorineural deafness. ENT-Ear, Nose, & Throat Journal. 2005, 84(1):14-5.
15. Mabrie DC, Niparko JK. Quiz Case 1. Meningitis-related labyrinthitis ossificans. Arch Otolaryngol Head Neck Surg. 1999, 125(8):912-4.
1. ENT doctor (Post-graduation student in Head and Neck Surgery at HSPE-SP).
2. 2nd yr. Resident Doctor in ENT and Head and Neck Surgery at HSPE-SP).
3. ENT Doctor (Assistant doctor in the Otology Department at HSPE-SP).
4. PhD in Otorhinolaryngology by UNIFESP (Head of ENT and Head and Neck Surgery Department at HSPE-SP).
Hospital do Servidor Público Estadual de São Paulo - FMO. Departamento de Otorrinolaringologia e Cirurgia de Cabeça e Pescoço.
Address:
Leandro Ricardo Mattiola.
Rua José de Magalhães 600 - Vila Clementino
São Paulo - SP - CEP 04026-090
Phone/Fax: (11) 5088-8406 - E-mail: lmattiola@hotmail.com
This article was submitted to SGP (Sistema de Gestão de Publicações - Publication Management System) of R@IO on May 31st, 2007 and approved on November 8th, 2007 at 00:33:58.
|
|
 |
|
|
