|
590 |
|
| Year: 2009 Vol. 13 Num. 1 - Jan/Mar - (10º)
|
|
 |
| Section:
Original Article
|
|
|
|
|
| Relation between Arterial Hypertension and Hearing Loss |
|
| Author(s): |
| Maria Fernanda Capoani Garcia Mondelli1, Andréa Cintra Lopes1
|
|
|
| Key words: |
| hypertension, hearing loss, tinnitus |
|
|
 |
| Abstract: |
Objective: To verify the relationship between systemic arterial hypertension (SAH) and hearing loss in middle-aged patient. Method: This study was carried out in the period from January to December 2007. The research was composed by 392 patients of both genders, aged from 45 to 60 years old. Anamnesis and threshold tonal audiometry data were analyzed. Results: There was a significant association between SAH and hearing loss. Conclusion: The results showed an evident association between SAH and hearing loss, which requires the disclosure of a preventive process.
|
|
|
INTRODUCTION
The hearing loss (HL) is a factor that irrespectively of the degree of commitment affects the quality of life of the people and when acquired in adults, it appears gradually and may make the oral language receiving difficult (1).
In the adult population, studies confirmed that HL starts at about 30 years old, and increases progressively along the years, although there is a resemblance in the audiologic configuration, men are affected earlier and more intensely than women (2). The hearing system affection may cause psychosocial effects, amongst which: low self-esteem, isolation, depression and irritability (3), and these problems interfere with the quality of life of the individuals (4). Moreover, it's known that metabolic changes, such as systemic arterial hypertension (SAH) is present in adults and may be empowered by the presence of hearing loss or vice-versa (5).
According to the data from SOB (Brazilian Society of Otology), (6), the HL somehow affects about 70% of the individuals, and it's then a public health matter, with specific needs as for the promotion of health and hearing rehabilitation.
Researchers (7) investigated 320 patients (160 men and 160 women) by means of anamnesis and tonal audiometry, their results confirmed that the audiologic and vestibular complaints were similar among both genders and in the audiometry they obtained hearing loss in the high frequencies for men, and among women, descendent and plane curves.
Studies confirm that hearing changes may derive from SAH and a few diseases are responsible for such frequent complications such as those arising out of arterial hypertension: cerebral vascular accident, cardiac, renal and peripheral vascular insufficiency (8).
Hypertension is taken as a silent disease for it doesn't present any symptom. However, some people present headache, dizziness, tinnitus, chest pain and weakness, which may be alert signals.
The SAH problem in Brazil is estimated by means of rates established in international works, and, based on the census projection of the Brazilian Institute of Geography and Statistics, there are today 90 million Brazilians aged over 20 years old. If we consider the prevalence of Arterial Hypertension to be of 20%, we conclude that at least, 18 million Brazilians are hypertensive, out of whom 50% ignore they have the disease (8).
All live cells need an adequate supply of oxygen and nutrients to maintain their functions and such supply depends upon the functional and structural integrity of the heart and bloody vessels (10). Therefore, the affection of the circulatory system may damage the inner ear functioning and from the physiopathologic mechanisms described it's the increase of blood viscosity that causes a diminishment of the capillary blood flow and oxygen transport (11).
The circulatory system pathology may affect the inner ear directly in several manners, damages a number of the auditory system abilities, and affects the acoustic or speech signal processing and consequently the individual's communication capacity (12), in addition to leading the patient to the presence of tinnitus (13-17).
The association between tinnitus and hearing loss has already been fully described. According to some works, 85 to 96% of the patients with tinnitus have some degree of hearing loss, and the prevalence of tinnitus increases along the aging years (18,19).
Tinnitus is considered a sound perception without its presence in the environment (20). It consists of a sensation defined as illusory and may be characterized as a noise similar to the sound of rain, sea, current water, bells, insects, whistle, squeaking, doorbell, pulsation etc. Such sensation may be continuous or intermittent, present with different tonal features, be intense or soft and is perceived in the ears or in the head (21,22).
The positive correlation of hearing loss to tinnitus may be justified if we take into account that the hearing loss is the tinnitus unleashing factor, since the damages or degenerations of the inner ear and the vestibulocochlear nerve may be its generators (20,22,23). Therefore it's reasonable to consider that the presence of hearing loss increases the risk for tinnitus to provoke interference with concentration and emotional balance or that it works as a co-factor of such interference, that is, the bothering note given to tinnitus is contaminated by the bothering caused by the associated hearing loss (23).
Many times the HL has been underestimated specially by professionals not bound to audiology. Then, the forwarding to audiologic evaluation are not made and the patient doesn't receive the rehabilitation benefits, which affect even more his or her quality of life.
Considering the hearing loss and arterial hypertension impact to the quality of life of the affected individuals, as well as the changes of cochlear activity that occur due to metabolic diseases, the objective of this study is to compare the results of anamnesis and threshold tonal audiometry of patients with and without arterial hypertension assisted at a high complexity center of hearing health.
METHOD
We accomplished a retrospective study in a high complexity center of hearing health. The project was approved by the Ethics Committee in the Institution Research under Protocol no. 101/2006-SVAPEPE-CEP.
The study included 392 individuals regularly enrolled at the high complexity service in hearing health, aged between 45 to 60 years old, evaluated from January to December 2007. The SAH diagnosis was determined by the general practitioner. It left out patients with previous history of specific auditory disorders, metabolic disorders, vascular disorders or those exposed to occupational noise, chemical products or who used ototoxic medication. The hearing was assessed by means of the conventional evaluation as described below.
The individuals' records were analyzed and the following proofs were considered:
Specific interview: was carried out as a closed set and contained information about the auditory and vestibular disorders symptomatology, presence of tinnitus, as well as exposure to hearing harmful agents, such as occupational or leisure noise, ototoxic drugs and general health conditions. Acoustic immittance measurements: carried out in order to evaluate the tympano-ossicular system, by means of tympanometric curve and acoustic reflexes research. Conventional Tonal Audiometry: researched frequencies belonging to the range from 0.25 to 8 KHz, for the airways and 500 to 4KHz for the osseous way, when the airways were equal or below 20dbNa. The equipment has corrections for standard Hearing Level ANSI S 3,6 - 1989, Safety norms IEC 642 and osseous vibrator B17, ANSI3.13, 1972 and ISO389, 1957/83. For the tonal thresholds researches we used the pure tone. Logoaudiometry: aimed at assessing the individual's capacity to identify and receive speech sounds. Such procedure was carried out by means of the same audiometer. Otoscopy: carried out by the otorhinolaryngologist. This procedure preceded the audiologic evaluation.
RESULTS
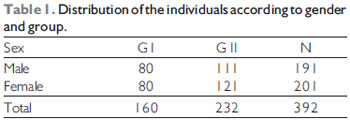
The study, composed by 392 participants, aged from 45 to 50 years old (average age 51.4 years old) was divided into 2 groups, G I, the hearing impaired without hypertension and GII, the hearing impaired with hypertension.
According to the objective of this study, the data obtained from both groups studied were compared according to: Degree and configuration of the hearing loss and anamnesis data.
We used the Mann-Whitney Chi-square Test (df=1) for comparison of the loss degree and the Chi-square Test (df=1) for comparison of the type of loss and presence of tinnitus.
The analysis of the individuals (n= 392) according to gender and group are distributed in Table 1.
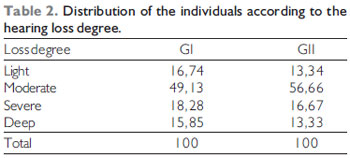
Table 2 indicates the analysis of the individuals according to the degree of hearing loss in the auditory impairment associated to systemic arterial hypertension (HL+SAH) and hearing loss (HL). We used the Mann-Whitney test (p-level 0.721434).
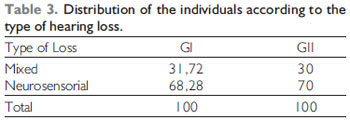
The analysis of the individuals according to the type of hearing loss in the groups of hearing loss associated to the systemic arterial hypertension (HL-SAH) and hearing loss (HL) is described in Table 3. We used the Chi-square Test 0.25 p=0.6177.
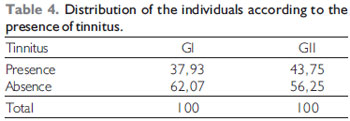
Table 4 offers the analysis of the individuals according to the presence of tinnitus in the hearing loss groups associated to systemic arterial hypertension (HL+SAH) and hearing loss (HL). We used the Chi-square Test 1.33 p=0.2483.
DISCUSSION
Today, the hearing loss (HL) associated with the systemic arterial hypertension (SAH) has been studied in populations diagnosed with noise-induced hearing loss (NIHL) (24), or presbyacusis - hearing loss resulting from aging.
The study demonstrated the existence of association between hearing loss and arterial hypertension with 232 individuals (Table 1), because, with aging, there is an increase of the number of chronic diseases (14), data that match those of other researchers (1, 27).
As for the gender, there was no statistically significant difference. Several works have been approaching the theme of gender and hearing loss concerning age (15, 17), but it was not possible to determine a correlation between these features in this work, as observed in Table 1.
As for the hearing loss degree, it was possible to observe a significant predominance of the moderate degree (Table 2), and the same occurred in a research accomplished with 552 exams of hypertensive patients, aged from 14 to 84 years old, and out of these, 43.06 presented with moderate loss (28).
Researchers associate the neurosensorial HL to a microcirculatory insufficiency resulting from a vascular occlusion by embolism, hemorrhage or vasospasm, and that these would be products of a diabetes or hypertension hyperviscosity or microangiopathy syndrome, which suggest hypertension could, through such factors, cause a HL (26); before the findings obtained with this study (n 392), out of 160 participants with arterial hypertension (G I), 210 ears were diagnosed with neurosensorial HL, data that may be observed in Table 3 and is opposite to the research of authors (25), who evaluated 50 patients with arterial hypertension and found 62% of neurosensorial hearing loss in this population.
The presence of tinnitus was reported by 37.93% of GI and 43.75% of GII, as indicated in Table 4, and there is no statistically significant difference between the individuals with and without SAH. Tinnitus is considered to be a symptom and not a disease and the etiological mechanism is still uncertain; some studies state it may occur as a consequence of an altered neural activity, resulting from a lesion or disorder in any level of the auditory system (21). Other authors suggest the tinnitus may occur due to metabolic abnormalities, high levels of cholesterol, cranial traumatisms and vascular problems (20).
Environmental factors to which mankind may be submitted such as noise, toxic substances inhaling, circulatory and metabolic alterations, in addition to infections, traumas of several natures and heredity may also influence the individual's hearing, and many times accelerates the degeneration process of the auditory system (13,18). We adopted exclusion criteria in this study - individuals who work or had worked in noisy places, with diabetes, history of interment or ingestion of ototoxic medicines; but it's known in the urban centers there is a large exposure to environmental noises, depending on the house, work, leisure location that end up providing the individual with an excessive and prolonged noise that certainly accelerates the auditory aging process, which justifies the age limit, although the literature states presbyacusis may start from the fourth decade of life.
The strict relation between SAH and HL in the adult population motivated this association research, by confirming that chronic diseases determined by genetic problems, lifestyle, environment and aging begin to be the main health problems of individuals after 45 years of age, aiming at increasing the number of individuals healthy and able to maintain the maximum of their physical and mental functions, with special attention given to those with systemic diseases, such as hypertension (29).
CONCLUSION
The hypertensive individuals didn't present with a strong hearing affection, and the HL degree and type are similar in both groups. As for the complaint of tinnitus, the group of individuals with SAH presented a higher occurrence.
The systemic arterial hypertension is an independent risk factor for hearing loss, therefore, it's important to disclose the need for preventive processes to minimize the degeneration mechanisms of the auditory system caused by circulatory problems, specially by arterial hypertension, as well as prioritize the early diagnosis of HL in people with SAH.
BIBLIOGRAPHICAL REFERENCES
1. Marchiori LLM, Filho EAR, Matsuo T. Hipertensão como fator associado a perda auditiva. Rev Bras Otorrinolaringol. 2006, 72(4):533-40.
2. Megighian D, Savastano M, Salvador L, Frigo A, Bolsan M. Audiometric and epidemiological analisys of elderly in the Veneto region. Gerontology. 2000, 46:199-204.
3. Bance M. Hearing and Aging. CMAJ. 2007, 176(7):925-7.
4. Yueh B, Shekelle P. Quality indicatores for the care of hearing loss in vulnerable elders. JAGS. 2007, 55:5335-39.
5. Mor R, Fragoso M, Figueiredo JM, Taguchi CK. Vestibulometria e fonoaudiologia. São Paulo: Lovise; 2001.
6. Sociedade Brasileira de Otologia-SBO. Otologia lança campanha da audição. 2005. Disponível em: www.sbotologia.com.br/09asp. acesso em 02/10/08.
7. Carmo LC, Silveira AM, Marone SAM, DOttaviano FG, Zagati LL, Lins EMDS. Estudo audiológico de uma população idosa brasileira. Rev Bras Otorrinolaringol. 2008, 74(3):342-349.
8. Toscano-Barbosa E. Expectativas para a abordagem da hipertensão no Brasil, com a mudança do século. Rev Bras Hipertens. 2000, 7(1):7-10.
9. Bersusa AAS. Hipertensão arterial: o que saber? Rev. Paul. Enfermagem. 2000, 19(3):32-40.
10. Marková M. The cochleovestibular syndrome in hypertension. Cesk Otolaryngol. 1990, 39(2):89-97.
11. Bachor E, Selig YK, Jahnke K, Rettinger G, Karmody CS. Vascular variations of the inner ear. Acta Otolaryngol. 2001, 121(1):35-41.
12. Moore B. Perceptual consequences of cochlear hearing loss and their implications for the design of hearing aids. Ear Hear. 1996, 17(2):133-61.
13. ASHA (American Speech- Language- Hearing Association). Disponível em www.asha.org. Acesso em 16/08/2006.
14. Baraldi GS, Almeida LC, Borge ACLC. Hearing loss and hypertension: findings in an older by group. Rev Bras Otorrinolaringol. 2004, 70(5):604-4.
15. Cruickshanks KJ, Wiley TL, Tweed TS, Klein BEK, Klein R, Mares-Perlman JA et al. Prevalence of hearing loss in older adults in Beaver Dam, Wisconsin. The Epidemiology of Hearing Loss Study. Am J Epidemiol. 1998, 148 (9):879-886.
16. Dan IB, Iório MCM. Dificuldade e desvantagem auditivas:estudo em idosos na adaptação de prótese audtiva. Rev Fono Atual. 2004, 50-4.
17. Lee FS, Matthews LJ, Dubno JR, Mills JH. Longitudinal Study of Pure-Tone Thresholds in Older Persons. Ear & Hearing. 2005, 26(1):1-11.
18. Marchiori LLM, Gibrin PCD. Diabetes mellitus: prevalence of hearing disorders. Arq Bras Endocrinol Metab. 2003, 47:82-6.
19. Sanchez TG, Ferrari GMS. O controle do zumbido por meio de prótese auditiva: sugestões para otimização do uso. Pró-Fono Revista de Atualização Científica. 2002, 14(1):111-8.
20. Elisabetsky M. Zumbidos: etiopatologia, diagnóstico e tratamento. Folha Méd. 1986, 93(5/6):323-332.
21. Fukuda Y. Zumbido: diagnóstico e tratamento. RBM-ORL. 1997, 4(2):39-43.
22. Fukuda, Y. Zumbido e suas correlações otoneurológicas. In: Ganança, M. Vertigem Tem Cura? São Paulo, Lemos Editorial, 1998, 171-176.
23. Sanchez TG, Medeiros IRT, Levy CPD, Ramalho JRO, Bento RF. Zumbido em pacientes com audiometria normal: caracterização clínica e repercussões Rev Bras Otorrinolaringol. 2005, 71(4):427-31.
24. Cordeiro R, Lima-Filho EC, Nascimento LCR. Noise-induced hearing loss and its association with cumulative working time among urban bus workers. Cad. Saúde Pública [serial on the Internet]. 1994 June [cited 2008 July 10] 10(2):210-221. Available from: http://www.scielosp.org/scielo.
25. Brohem VM, Caovilla HH, Ganança MM. Dos sintomas e achados audiológicos e vestibulares em indivíduos com hipertensão arterial. Acta Awho. 1996, 15(1):4-10.
26. Carrasco VN, Prazma J, Faber JE. Cochlear microcirculation effect of adrenergic agonists on arteriole diameter. Arch Otolaryngol Head Neck Surg. 1990, 116:411-7.
27. Marchiori LLM, Filho EAR. Queixa de vertigem e hipertensão arterial. Rev CEFAC São Paulo, 2007 9(1):116-21.
28. Marchiori LLM, Freitas SV, Vieira M. Análise de prevalência das queixas e perdas auditivas de pacientes com hipertensão arterial submetidos à avaliação audiológica. Fono Atual. 2002, 21:97-104.
29. Teixeira AR, Freitas CR, Millão LF, Gonçalves AK, Berker Junior B, Vieira AF, Farias EM, Martins CR, Santos AMPV, Lopes PTC, Martins IA, Pol DOC, Gonçalves CJS. Relação entre deficiência auditiva, idade, gênero e qualidade de via de idosos. Arq. Int. Otorrinolaringol. 2008, 12(1):62-70.
1. Doctor. Professor - Doctor at FOB/USP.
Institution: Divisão de Saúde Auditiva / HRAC-USP Bauru. Bauru / SP - Brazil.
Mail address:
Maria Fernanda Capoani G. Mondelli
Departamento de Fonoaudiologia
Faculdade de Odontologia de Bauru
Alameda Octávio Pinheiro Brizola 9-75 - Vila Universitária Bauru
São Paulo - Brazil - Zip code: 17012-901
Telephone: (+55 14) 3235-8232.
Article received on December 15, 2008.
Approved on March 12, 2009.
|
|
 |
|
|