 |
616 |
|
| Year: 2009 Vol. 13 Num. 2 - Abr/Jun - (14º)
|
|
 |
|
|
| Giant Osteoma of the Ethmoidal Sinus |
|
| Author(s): |
| Otavio Marambaia1, Amaury de Machado Gomes2, Pablo Pinillos Marambaia3, Maili Pinheiro4, Fabio Siqueira Costa Almeida5
|
|
|
| Key words: |
| ethmoidal, giant, osteoma, sinus. |
|
|
 |
| Abstract: |
Introduction: The osteomas are osseous lesions with slow and asymptomatic growth that most of the times is a finding in radiological exams requested for other reason. It's the most common benign neoplasm of the paranasal sinuses. The osteomas are located mainly in the frontal sinus (57% to 80%), followed by the ethmoidal sinuses (20%), maxillary sinuses and rarely in the sphenoid sinus. It has a discreet predominance in the male sex 1.5 and its incidence is higher in the 3rd and 4th decades of life. The treatment is surgical no matter the size. Objective: To describe a case of giant osteoma of the ethmoidal sinus including a brief literature review. Case Report: JDA, male, 33 years old, presented with a right constant nasal obstruction for 01 year. Upon exam, he presented with facial asymmetry with lateralization of the right ocular globe. The computed tomography of the paranasal sinuses showed a lesion with density of soft parts occupying partially the right nasal cavity, ethmoid sinus and right maxillary. The patient was submitted to surgery with full exeresis of the lesion. The anatomopathological exam confirmed osteoma. The patient evolved without evidences of the lesion recurrence. Final Comments: The osteomas in the ethmoidal sinus, irrespectively of the size and due to the risk of complications, must be operated.
|
|
|
INTRODUCTION
Osteomas are osseous lesions of slow growth that may affect the paranasal sinuses and most of the times are asymptomatic, and they are a finding in radiological exams requested for other reason (1,2,3,4,7). The osteoma is the most frequent benign neoplasm of the paranasal sinuses (1,2,7), and is located mainly in the frontal sinus (57 to 80%) (1,2,3,4,6,7), followed by the ethmoidal sinuses (20%) (1,3). It presents a discreet predominance in the male sex, 1.5, and its occurrence is higher in the 4th decade of life (1,3,4,5). The treatment is surgical (1,3,5). This report describes one case of giant osteoma of the ethmoidal sinus.
CASE REPORT
JDA, male, black, 33 years old, sought the otorhinolaryngology service with a history of constant nasal obstruction to the right for 01 year. He denied epistaxis and rhinorrhea. He presented a discreet right facial asymmetry associated with the case. Upon exam, he presented with facial asymmetry with lateralization of the right ocular globe. The nasal endoscopy revealed a hardened mass coming from the lateral wall at the right side that partially occupied the nasal cavity light at this side. The computed tomography of the paranasal sinuses showed a radiopaque and heterogeneous lesion, with areas of density of soft parts inside it, with well defined limits, partially occupying the right nasal cavity, ethmoidal sinus and right maxillary, with a possible affection of the papyraceous lamina of this side. (Pictures 1 and 2). The patient was submitted to surgery through the external surgical access by means of lateral rhinotomy with supra-orbitary extension (Picture 3), under general anesthesia, and the osseous tumor was fragmented with an air motor drill with full exeresis of the lesion. The anatomopathological exam confirmed the suspicion of osteoma (Picture 4). The patient evolved without evidences of the lesion recurrence (Picture 5).
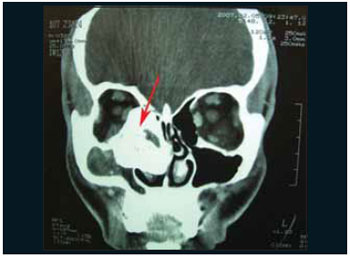 Picture 1. Computed tomography of face, coronal cut, radiopaque and heterogeneous lesion, with areas of density of soft parts inside it, with well defined limits, partially occupying the right nasal cavity, ethmoidal sinus and right maxillary, with a possible affection of the papyraceous lamina of this side.  Picture 2. Computed tomography of face, axial cut, radiopaque and heterogeneous lesion, with areas of density of soft parts inside it, with well defined limits, partially occupying the right nasal cavity, ethmoidal sinus and right maxillary, with a possible affection of the papyraceous lamina of this side.  Picture 3. Intraoperative picture. Removal of ethmoidal osteoma by using lateral rhinotomy with supra-orbitary extension. 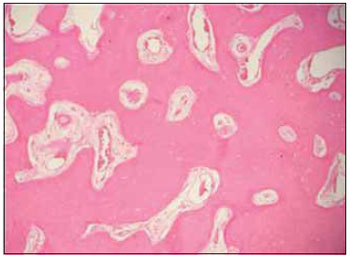 Picture 4. Picture of the Lamina. Histological cut showing osseous trabecula penetrated by stroma containing fibroblasts (HE x 100).  Picture 5. CT of face, coronal cut, postoperative.
DISCUSSION
Osteoma is the most common benign tumor of nose and paranasal sinuses (1,2,3,4,7). Its incidence varies from 0.43% to 3% (2,3,4,7), and it's generally located in the frontal sinus (57-80%) (1,3,4,6,7) followed by the ethmoidal sinuses (16-25%) (3). In this specific case the giant osteoma affected the right ethmoidal and maxillary sinus. They are more frequent in the male sex and in the 4th decade of live (1,3,4,5,7).
Most osteomas are asymptomatic (5,7). The most frequent symptom in patients with osteomas of ethmoidal sinuses is frontal headache of facial pain (53%) (1,2,3,4,6,7), frequently secondary to ostium obstruction or infection of the sinus. Our patient only presented nasal obstruction on the right side, as well as facial asymmetry without, however, presenting diplopia or reduction of visual accuracy.
The diagnosis is made through simple X-ray and Computed Tomography of the paranasal sinuses (3,4,5,7). The differential diagnosis includes ossifying fibroma, osteosarcomas, mucoceles and polyps (4,7).
The surgical indication of the osteomas of frontal and ethmoidal sinuses was reviewed by Savic and Djeric in 1990 and they suggested that all osteomas should be operated when overtaking the frontal sinus limits, in the presence of infection and in all cases of ethmoidal osteomas, irrespectively of their size (1,7), for the risk of complications. In this specific case, we used side rhinotomy with access from supra-orbitary extension. The choice of the approach way must take into account the size, location and extension of the lesion, however, we must mostly prevent aesthetic deformities (1,7).
Today the endoscopic access has been used for the treatment of small ethmoidal osteomas, without extrasinusal extension (1,6,7). Our patient was submitted to surgery externally, the osseous tumor was fragmented with an air motor drill and the patient evolved without sequels.
FINAL COMMENTS
The osteomas of the paranasal sinuses are benign osseous lesions generally asymptomatic and sometimes large lesions may be unrealized until they reach large proportions. However, those located in the ethmoidal sinus, irrespectively of the size and due to the risk of complications, must be operated.
BIBLIOGRAPHICAL REFERENCES
1. Balieiro OF, Bordash A, Stamm A, Sebusiani BB, Baraúna I. Abordagem Cirúrgica para os Osteomas dos Seios Paranasais. Rev Bras Otorrinolaringol. 2004, 70(2):164-170.
2. Huang HM, Liu CM, Lin KN, Chen HT. Giant Ethmoid Osteoma with Orbital Extension, a Nasoendoscopic Approach Using an Intranasal Drill. Laryngoscope. 2001,111.
3. Carvalho C, Schellini S, Tagliarini JV, Nakajima V, Domingues MA. Osteoma do Etmóide com Invasão Orbitária: Relato de Três Casos e Revisão da Literatura. Arq Bras Oftalmol. 2007, 70(6):1024-1028.
4. Fobe LPO, Melo EC, Cannone LF, Fobe JL. Cirurgia de Osteoma de seio Frontal. Arq Neuropsiquiatr. 2002, 60(1):101-105.
5. Zouloumis L, Lazarides N, Papadaki M, Epivatianos A. Osteoma of the Ethmoidal Sinus: A Rare Case of Recurrence. British Journal of Oral and Maxillofacial Surgery. 2005, 43:520-522.
6. Panagiotopoulos V, Tzortzidis F, Partheni M, Iliadis H, Fratzoglous M. Giant Osteoma of the Frontoethmoidal Sinus Associated with Two Cerebral Abscesses. British Journal of Oral and Maxillofacial Surgery. 2005, 43:523-525.
7. Tiago RSL, Melo ECM, Fobé LPO. Osteomas fronto-etmoidais: aspectos clínicos e cirúrgicos. Rev Bras Otorrinolaringol. 2002, 68(4):516-520.
1. Otorhinolaryngologist - ABORL. Coordinator of the INOOA Otorhinolaryngology traineeship program Professor of the Discipline of Otorhinolaryngology of the Escola Bahiana de Medicina e Saúde Pública - EBMSP.
2. Otorhinolaryngologist - ABORL. Preceptor of the Inooa's Otorhinolaryngology Service.
3. Otorhinolaryngologist - ABORL. Assistant Doctor - Inooa.
4. Trainee Doctor of the 3rd Year - Inooa.
5. Medicine. Resident.
Institution: Instituto de Otorrinolaringologia Otorrinos Associados - Inooa. Salvador / BA - Brazil.
Mail address:
Otavio Marambaia
Avenida ACM, 2603 - Ed. Ventura de Matos
Salvador / BA - Brazil - Zip code: 40280-000
Telephone: (+55 71) 3270-8000 - Fax: (+55 71) 3270-8020
E-mail: otaviomarambaia@hotmail.com
Article received on December 12 2007.
Approved on August 23 2008.
|
|
 |
|
|
