|
631 |
|
| Year: 2009 Vol. 13 Num. 3 - Jul/Set - (10º)
|
|
 |
| Section:
Original Article
|
|
|
|
|
| Occupational Hearing Loss: Tonal Audiometry X High Frequencies Audiometry |
|
| Author(s): |
| Andréa Cintra Lopes1, Karina Aki Otubo2, Talita Costa Basso3, Érica Juliana Innocenti Marinelli3, José Roberto Pereira Lauris4.
|
|
|
| Key words: |
| noise induced hearing loss, audiometry, hearing, occupational noise. |
|
|
 |
| Abstract: |
Introduction: Studies on the occupational exposure show that noise has been reaching a large part of the working population around the world, and NIHL (noise-induced hearing loss) is the second most frequent disease of the hearing system. Objective: To review the audiometry results of employees at the campus of the University of São Paulo, Bauru. Method: 40 audiometry results were analyzed between 2007 and 2008, whose ages comprised between 32 and 59 years, of both sexes and several professions: gardeners, maintenance technicians, drivers etc. The participants were divided into 2 groups: those with tonal thresholds within acceptable thresholds and those who presented auditory thresholds alterations, that is tonal thresholds below 25 dB (NA) in any frequency (Administrative Rule no. 19 of the Ministry of Labor 1998). In addition to the Conventional Audiologic Evaluation (250Hz to 8.000Hz) we also carried out High Frequencies Audiometry (9000Hz, 10000Hz, 11200Hz, 12500Hz, 14000Hz and 16000Hz). Results: According to the classification proposed by FIORINI (1994), 25.0% (N=10) they presented with NIHL suggestive audiometric configurations. The results of high frequencies Audiometry confirmed worse thresholds than those obtained in the conventional audiometry in the 2 groups evaluated. Conclusion: The use of high frequencies audiometry proved to be an important register as a hearing alteration early detection method.
|
|
|
INTRODUCTION
When we think of the diversity of health problems generated by the productive processes, there emerges the need for experiences that find the understanding of health aggravation provoked by the work in social groups. The speed of changes of these productive processes involves the appearing of risk situations due to the implementation of new technologies and manners of work organization and, therefore, a change to the health standard of the working class (1).
We may consider to be an important factor of this process the increase of pollution rates, mainly in the big cities. Given the third major cause of environmental pollution, behind water and air pollution (2), the noise is the most frequent physical agent harmful to health in the work environment, and is characterized as a the factor of most prevalence for the origin of occupational diseases (3). The intense noise occupational exposure may be characterized as an acoustic trauma (sudden loss, resulting from a single exposure to intense noise), threshold temporary alteration (audibility threshold elevation that is recovered gradually after exposure to noise) and PAINPSE
-High Pressure Levels Induced Hearing Loss (characterized by the degeneration of hair cells of the Corti's Organ) (2,4,5).
In Brazil, PAINPSE is known to represent one of the most frequent diseases among our workers, and is the second major cause of hearing loss in adults, second only to presbycusis (6). PAINPSE is defined as the hearing loss generated by high sound pressure levels, with alterations of the auditory thresholds, of neurosensorial, generally bilateral type, resulting from occupational noise exposure, and its main features include irreversibility and gradual progression with the time of risk exposure (7). Its natural history initially shows the affection of the auditory thresholds in one or more frequencies ranging from 3000Hz to 6000Hz. The other frequencies may lead longer to be affected. Once ceased the exposure, there will be no progression of the hearing reduction (8,9,10,11).
25% of the exposed working population is estimated (12,13,14,15) to have PAINPSE in some degree. In spite of being the most frequent aggravation to the workers' health, its prevailing data are not yet much known in Brazil. This reinforces the importance of notification that enables the awareness of the reality and dimensions the required prevention and assistance measures (2).
Once there is no clinical treatment for this kind of hearing loss, the prevention of the problem is very important with adoption of environmental actions, associated to the use of individual protection equipment; even though the legislation in force in Brazil has not been avoiding the dissemination of the professional deafness (16,17).
In the literature researched, it was necessary to investigate the auditory health conditions of workers at the University of São Paulo, Bauru campus, allocated in environments whose level of sound pressure exceeds 80dBNPS (action level), comprising hearing losses prevention programs, aiming to minimize the risks of occupation origin auditory deficiency and then enabling the maintenance of the auditory quality of the respective individuals.
METHOD
This study relied on the participation of the employees of the University of São Paulo who remain exposed to environmental noise at intensity above 80 dBNPS (action level), during the day's work of 8 hours, located at the University Campus of Bauru, and are periodically submitted to Audiological Assessment. This assessment is part of the (PPRA) Environmental Risks Prevention Program and the (PCMSO) Program for Medical Control and Occupational Health, set up by the Institution's (SESMIT) Specialized Service of Work Safety and Medicine.
40 periodical results of audiometry carried out between 2007 and 2008 were analyzed in the Phonoaudiology Clinic of the College of Odontology of Bauru FOB/USP, out of which 70% were composed by the male sex (N=28) and 30% of the female sex (N=12), aged between 32 and 59 years, whose professions varied among: laundry, gardeners, maintenance technicians, cabinet-makers, machine operators and drivers.
The study model adopted was of retrospective type and characterized by the division of participants exposed to occupational noise in 2 groups: GROUP I - those with tonal thresholds within the acceptable limits, the cases whose audiograms show auditory thresholds lower or equal to 25 dB(NA), in all frequencies examined; and GROUP II -considered to be suggestive of auditory loss induced by high sound pressure levels the cases whose audiograms, in the frequencies of 3000 and/or 4000 and/or 6000 Hz, had auditory thresholds above 25 dB(NA) and higher than in the other frequencies tested, whether they were committed or not (7).
For survey of data regarding the clinical and occupational history of the participants, a specific interview was carried out by means of a questionnaire. With exclusion criteria the following factors were determined: a) Presenting neurological, psychiatric and/or cardiac problems; b) Using ototoxic medication; c) Presenting auditory deficiency with a determined etiology that is not PAINPSE. After the interview, the (MAE) External Acoustic Meatus Inspection was performed aiming at verifying possible commitments that could interfere with the specific evaluations, such as, occlusion of the canal resulting from wax. In the data collection the Siemens trademark audiometer, model SD50 was used with auricular phones HAD 200, Vibrasom acoustic cabin, and was duly calibrated by meeting the norms of audiometer gauging according to INMETRO.
In addition to (AT-AC) Conventional Threshold Tonal Audiometry, whose frequencies analyzed comprise the ranges from 250Hz to 8000Hz, the (AT-AF) High Frequencies Tonal Audiometry was also used because according to studies carried out, it is an early diagnosis instrument for auditory alterations resulting from some etiological agents, such as, levels of high sound pressure levels (18).
The data collected were stored in a software (Microsoft Excel) for further statistical analysis. In all the statistical tests the level of significance of 5% (p < 0.05) was adopted as suggested for biological studies. The descriptive statistics was used by means of averages, medial rate, minimum and maximum values. In the analysis of difference between the averages the paired t-test was used, and for correlation of the frequencies with exposure age and time the Pearson's coefficient was used.
Research approved by the Ethics Committee in Research of the College of Odontology of Bauru FOB/USP under protocol no. 030 / 2007, whose Free and Clarified Authorization Terms of the participants are attached to their respective records.
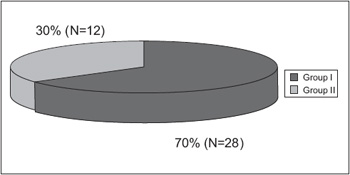 Graphic 1. Workers auditory profile (according to the Administrative Rule no. 19 of the Ministry of Labor and Employment - 1998).
RESULTS
The analysis of the 40 audiometries (80 ears) allowed the characterization of the auditory profile of workers who are exposed to noise (Graphic 1). Group I (70%), composed by the individuals with results of tonal audiometry within acceptable limits, obtained a major prevalence compared to Group II (30%), whose audiograms, in the frequencies of 3000 and/or 4000 and/or 6000 Hz, presented auditory thresholds above 25 dB (NA) and higher than in the frequencies tested (7).
Seeking to obtain a more specific classification for these findings, we used as reference the classification proposed in the literature (19), and found 27.5% (N=11) of normal audiometry (all thresholds equal or lower than 25dB (NA)), 45% (N=18) whose audiograms were normal with incision (lowering in one of the frequencies of 3, 4 or 6 kHz, with difference of at least 10dB compared to the anterior or posterior frequency), and 25.0% (N=10) audiometric drawing suggestive of noise induced hearing loss (auditory thresholds above 25dB (NA) in the range of frequency from 3 to 6 kHz), whose results are concerning when compared to other studies (19,20,32) because they are similar to the data found in industry workers (23.7%) and truck drivers (28.6%). In the performance of this analysis 39 exams were considered due to the occurrence of 2.5% (N=1) of unilateral light hearing loss (right ear).
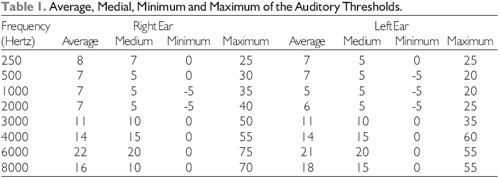
As well as the studies about PAINPSE (8,9,10,11) point out that the auditory thresholds are initially affected in one or more frequencies of the range of 3000Hz to 6000Hz, the values found in this study proved that in addition to confirming such findings, the frequency of 6000 Hz was mostly affected (Table 1).
Considering the general average of the two groups involved (based on Administrative Rule no. 19 of the Ministry of Labor and Employment - 1998), for the frequencies of 500Hz, 1000Hz and 2000Hz, we obtained the average of 6 dB for the left ear and 7 dB for the right ear. The average found for frequencies of 3000 Hz, 4000 Hz and 6000 Hz, was of 15 dB for the left ear and 16 for the right ear. In addition to the Conventional Audiometry (250Hz to 8000 Hz), we also performed the High Frequencies Tonal Audiometries (9000Hz, 10000Hz, 11200Hz, 12500Hz, 14000Hz e 16000Hz), whose results indicated the average of the left and right ears were of 28 dB. The comparison between the auditory thresholds averages of the right and left ears carried out by means of the paired t-test did not present any statistically significant differences for the high frequencies (p = 0.957), as well as for the low frequencies (p = 0.238).
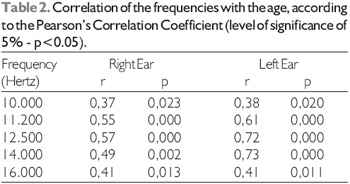
In the investigation of correlation between the age of the participants with tonal thresholds (Table 2), we confirmed that the (AT-AF) High Frequencies Tonal Audiometry presented significant values compared to the (AT-AC) Conventional Tonal Audiometry Frequencies.
When the correlation between time of work exposed to noise and the audiometric thresholds (N = 30) were researched, we verified a positive and significant correlation in the frequencies of 9000 Hz for the right ear (r= 0.38 p=0.037), and 14000 for the left ear (r= 0.26 p=0.165). The results confirmed that the two groups studied (with results of tonal audiometry within the acceptable limits, and those whose results presented alterations in the auditory thresholds, that is, tonal threshold below 25 dB (NA) in the frequencies of 3000 and/or 4000 and/or 6000 Hz and higher the in other frequencies tested, whether they were affected or not) (7), had worse responses in the high frequencies audiometry, which then showed that the use of this record seems to be important as an early detection method of auditory alterations.
The own PAINPSE is characterized by a constellation of signs and symptoms that go beyond a hearing loss and may not be limited to a simple quantitative loss of the auditory sensitivity (21). Among the auditory complaints found with major occurrence (Graphic 2), we find tinnitus, followed of headache, dizziness, otorrhea and otalgia. A study carried out (22,23) found similar symptoms in metallurgic workers and there was a major prevalence of complaints of difficulty for speech perception, hypacusis, tinnitus, sensation of auricular plenitude, otorrhea and dizziness. In the cases found in workers of the city of Bauru (24), the prevalence of tinnitus (48%) in the 284 workers exceeded the findings of another study (25), 28% of the cases, because according to the authors, the symptom subjectivity is a factor of higher difficulty and scarcity of data in the study of tinnitus.
The precedence relating to acoustic trauma were not considered to be relevant because they were reported in only 2 cases (5%), but the exposure to chemicals, 30%, followed of the exposure to vibration and heat (20%), and work accident (10%), contribute for the findings of important relevance in the area which the factors that contribute in the auditory sensitivity regard. The literature presents several works that show the existence of auditory lesion as a result from occupational exposure to Chemicals (PQ), even in the absence of noise, and others that seek to demonstrate an interaction between noise and chemicals (12,26). According to some studies (27), the relative estimated risk for the development of hearing loss was of 10.9 for noise and toluene, considering that the data were found in workers of a graphic with a higher prevalence of hearing loss in high frequency (3000 to 8000 Hz, in the group exposed to noise and toluene 53%). However, the audiometric findings suggest the exposure associated between noise and chemicals potentializes the risk of hearing loss.
Due to high levels of sound pressure, there is the need for use of hearing protection devices by the workers (28). In this study, we obtained the following data about the use of the equipment:
The type of the mostly found IPE was that of insertion 8 (20%), followed by auricle 3 model (7.5%). A questionnaire carried out in a metallurgic industry (28) obtained results similar to the predominance of use of insertion type IPE.
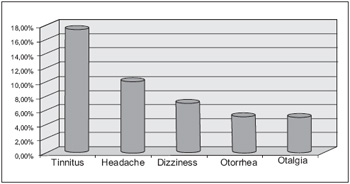 Graphic 2. Distribution of the auditory complaints found in the two groups studied.
 Graphic 3. Relation of the number of users (in percentage %), in the use of IPE - Individual Protection Equipment.
DISCUSSION
Before the audiological findings, we may observe that Group I (70%), whose results are within the acceptable limits, exceeded the number represented by Group II (30%); those which presented alterations in the auditory thresholds, that is, in the frequencies of 3000 and/or 4000 and/or 6000 Hz, presented auditory thresholds above 25 dB(NA) and higher than in other frequencies tested, whether they are affected or not (7).
By means of a specific classification (19), we found distinct results from the previous analysis because 27.5% (N=11) had normal audiometry (all the thresholds equal or lower than 25dB(NA)), 45.0% (N=18) presented normal audiograms with incision (lowering in one of the frequencies of 3, 4 or 6 kHz, with difference of at least 10dB compared to the earlier or later frequency), and 25.0% (N=10) audiometric drawing suggesting noise induced hearing loss (auditory thresholds above 25dB(NA) in the frequency range from 3 to 6 kHz). Alarming outcomes, since if only the first analysis was considered we would be leaving a large number of individuals behind a necessary attention.
We may also verify that the (AT-AF) High Frequencies Tonal Audiometry may contribute too much in the early findings of auditory alterations, by thus promoting a quick and efficient intervention in the combat to the wear the noise provokes in the worker's auditory and general health. Nevertheless, the AT-AF must not be measured for diagnosis for the fact there is not a normality standard established. However, when the individual audiometry is carried out prior to the deleterious exposure, the monitoring and early diagnosis of ototoxicity and lesions induced by high levels of sound pressure is fully feasible and reliable, and is based on the initial individual auditory thresholds to perform a comparative analysis (29).
As we have verified in several studies (5, 20, 23, 30, 31, 32), the correlation between the age and time of exposure are factors that have influenced the worsening of these workers' auditory threshold because according to the increase of age and time, the audiometry presented with some altered frequencies.
The non-auditory complaints were found similar to other researches (22, 24, 25), with the predominance in the number of cases of tinnitus, 17.5% (N=7), followed by headache 10% (N=4); dizziness 7% (N= 3), and otorrhea and otalgia 5% (N= 2). The findings on the use of Individual Protection Equipment (EPI), were also considered to be preoccupying because out of 40 individuals researched, only 25% (N=10) use it during the day's work, 2.5% (N=1) used it asystematically and most of whom, 62.5% (N=25) did not use it. Considering the importance and the efficacy the use of IPE may offer to the worker and also the findings of our research, we may realize that the awareness will be the best way to be adopted, but the regular use, as well as the hygienization and lifetime must be clarified for the general working population so as to achieve the highest number of people, by thus contributing for the auditory conservation and quality of the individuals exposed.
CONCLUSION
This study allowed us to confirm:
- According to the classification proposed in the literature (19), 25% of the audiograms were considered to be suggestive of PAINPSE;
- The mostly affected frequency was that of 6000 Hz;
- The age and time of exposure favored the lowering of the auditory thresholds;
- High Frequency Audiometry is a favorable instrument for the early detection of auditory thresholds alterations.
FINAL CONSIDERATIONS
This study confirmed that the scientific research has a lot to contribute to these workers auditory health quality, by innovating and multiplying the information in search of a more favorable and safe work environment.
BIBLIOGRAPHICAL REFERENCES
1. Lima MIM, Câmara VM. Uma metodologia para avaliar e ampliar o conhecimento de adolescentes do ensino fundamental sobre acidentes de trabalho. Cad. Saúde Pública. 2002, 18:115-20.
2. Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Ações Programáticas Estratégicas. Perda auditiva induzida por ruído (Pair)-(Série A. Normas e Manuais Técnicos) (Saúde do Trabalhador; 5. Protocolos de Complexidade Diferenciada) - Brasília: Editora do Ministério da Saúde, 2006. Disponível em: http://www.opas.org.br/ saudedotrabalhador/arquivos/Sala326.pdf
3. Padovani C, Nova CV, Queirós F, Sila LPA. Percepção das condições auditivas pelos servidores públicos da Universidade do estado da Bahia: considerações sobre o projeto saúde auditiva. Rev. Baiana de Saúde Pública. 2004, 28:203-11.
4. Hungria H. Otorrinolaringologia. Rio de Janeiro: Guanabara-Koogan; 1995.
5. Santos UP, Morata TC. Efeitos do ruído na audição. In: Santos UP (eds). Ruído: riscos e prevenção. São Paulo: Hucitec; 1994, pp.157.
6. Franks JR, Stephenson MR, Merry CJ. Preventing occupational hearing loss: a pratical guide. US: NIOSH; 1996.
7. Brasil. Portaria nº 19, de 09 de abril de 1998. Estabelece a necessidade de diretrizes e parâmetros mínimos para a avaliação e o acompanhamento da audição dos trabalhadores, expostos a níveis de pressão sonora elevados e o texto técnico. Ministério do Trabalho e Emprego, Brasília. Disponível em: http://www.mte.gov.br/legislacao/ portarias/1998/p_19980409_19.pdf
8. Melnick W.Tratado de Audiologia Clínica. In: Katz J. São Paulo: Manole; 1989.
9. Fernandes M, Morata TC. Estudo dos efeitos auditivos e extra-auditivos da exposição ocupacional a ruído e vibração. Rev. Bras. de Otorrinolaringol. 2002, 68:705-13.
10. Comitê Nacional de Ruído e Conservação Auditiva. Perda auditiva induzida por ruído relacionada ao trabalho. 1999. Disponível em: http://saudetrabalho.sites.uol.com.br/PAIR/ Perd_Aud_Ind_Ruido.pdf
11. American College of Occupational and Environmental Medicine; Acoeme Evidence Based Statement. Noise induced hearing loss. J. Occup. Environ. Med. 2003, 45.
12. Bergström B, Nyström B. Development of hearing loss during long term exposure to occupational noise. Scand. Audiol.1986, 15:227-34.
13. Carnicelli MVF. Audiologia preventiva voltada à saúde do trabalhador: organização e desenvolvimento de um programa audiológico numa indústria têxtil da cidade de São Paulo. São Paulo, 1988, p. 113. (Tese de Mestrado -Pontifícia Universidade Católica).
14. Morata TC. An epidemiological study of the effects of exposure to noise and organic solvents on workers hearing and balance. Cincinnati, 1990. (Tese de Doutorado University of Cincinnati).
15. Próspero AC. Estudo dos efeitos do ruído em servidores do Centro Técnico Aeroespacial. São Paulo, 1999, p. 119. (Tese de Mestrado - Pontifícia Universidade Católica).
16. Seligman J. Efeitos não auditivos e aspectos psicossociais no indivíduo submetido a ruído intenso. Rev. Bras. de Otorrinolaringol. 1993, 59:257-59.
17. Ogildo R, Costa EA, Machado HC. Prevalência de sintomas auditivos e vestibulares em trabalhadores expostos ao ruído ocupacional. Rev. Saúde Pública. 2009, 43:377-80.
18. Sayeb DR, Filho OAC, Alvarenga KF. Audiometria de alta frequência: estudo com indivíduos audiologicamente normais. Rev. Bras. de Otorrinolaringol. 2003, 69:93-9.
19. Fiorini AC. Conservação auditiva: estudo sobre o monitoramento audiométrico em trabalhadores de uma indústria metalúrgica. São Paulo, 1994. (Tese de Mestrado -Pontifícia Universidade Católica de São Paulo).
20. Lopes G, Russo ICP, Fiorini AC. Estudo da audição e da qualidade de vida em motoristas de caminhão. Rev. CEFAC. 2007, 9:532-42.
21. Costa EA. Desenvolvimento de teste de reconhecimento de fala, com ruído, em português do Brasil, para aplicação em audiologia ocupacional. Campinas, 1998. (Tese de Doutorado - Universidade Estadual de Campinas).
22. Araújo SA. Perda auditiva induzida pelo ruído em trabalhadores de metalúrgica.Rev. Bras. de Otorrinolaringol. 2002, 68:47-52.
23. Caldart AU, Adriano CF, Terruel I, Martins RF, Caldart AU, Mocellin M. Prevalência da Perda Auditiva Induzida pelo Ruído em Trabalhadores de Indústria Têxtil. Arq. Inter. de Otorrinolaringologia. 2006, 10(3):192-96.
24. Dias A, Cordeiro R, Corrente JE, Gonçalves CGO. Associação entre perda auditiva induzida pelo ruído e zumbidos. Cad. de Saúde Pública. 2006, 22:63-68.
25. Sanchez TG, Bento RF, Miniti A, Cârnara J. Zumbido: características e epidemiologia. Experiência do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo. Rev. Bras. Otorrinolaringol. 1997, 63:229-35.
26. Fechter L, Chen GH, Johnson D. Potentiation of noise induced hearing loss by low concentration of hydrogen cyanide in rats. Toxicological Sciences. 2002, 66:131-38.
27. Souza MMN, Bernardi AP. Ototoxidade dos produtos químicos: enfoque ocupacional. Rev. CEFAC. 2001, 3:95-102.
28. Gonçalves CGO. Implantação de um programa de preservação auditiva em metalúrgica: descrição de uma estratégia. Distúrbios da Comunicação. 2004, 16:43-51.
29. Sá LCB, Lima MAMT, Tomita S, Frota SMMC, Santos GA, Garcia TR. Avaliação dos limiares de audibilidade das altas frequências em indivíduos entre 18 e 29 anos sem queixas otológicas. Rev. Bras. Otorrinolaringol. 2007; 73:215-25.
30. Teles RM, Medeiros MPH. Perfil audiométrico de trabalhadores do distrito industrial de Maracanaú - CE. Revista da Sociedade Brasileira de Fonoaudiologia. 2007, 12:233-39.
31. Gonçalves CGO, Iguti AM. Análise de programas de preservação da audição em quatro indústrias metalúrgicas de Piracicaba, São Paulo, Brasil. Cad. Saúde Pública. 2006, 22:609-18.
32. Lopes AC, Nelli MP, Lauris JRP, Amorim RB, Melo ADP. Condições de saúde auditiva no trabalho: investigação dos efeitos auditivos em trabalhadores expostos ao ruído ocupacional. Arq. Inter. Otorrinolaringol. 2009, 13(1):49-54.
1. Doctor. Doctor Professor.
2. Phonoaudiologist. In college.
3. Phonoaudiologist.
4. Associate Professor of the Odontopediatrics, Orthodontics and Collective Health Department of FOB-USP. Associate Professor of the Odontopediatrics, Orthodontics and Collective Health Department of FOB-USP.
Institution: Faculdade de Odontologia de Bauru FOB/USP. Bauru / SP - Brasil. Mail Address: Andréa Cintra Lopes - Professora Doutora do Departamento de Fonoaudiologia da Faculdade de Odontologia de Bauru - Universidade de São Paulo - Alameda Dr. Octávio Pinheiro Brisolla, 9-75 - Vila Universitária - Bauru / SP - Brasil - CEP: 17043-101 - Postal Code: 73 Phone: (14) 3235-8000 ext.: 8557 - E-mail: aclopes@usp.br Pró-Reitoria de Cultura e Extensão Universitária USP
Article received on August 3 2009. Accepted on August 16 2009.
|
|
 |
|
|