 |
663 |
|
| Year: 2010 Vol. 14 Num. 1 - Jan/Mar - (3º)
|
|
 |
| Section:
Original Article
|
|
|
|
|
| Study of the Audiological' Profile of Individuals Attended in a Brazilian Diagnostic Service |
|
| Author(s): |
| Isabela de Souza Jardim1, Juliana Harumi Iwahashi2, Valéria de Campos Paula3.
|
|
|
| Key words: |
| hearing loss, tinnitus, dizziness, hearing, diagnosis. |
|
|
 |
| Abstract: |
Introduction: Hearing loss can affect the health and quality of life of the individual. The finding of the audio logical profile becomes important epidemiological tool for the explanation of new health policies, effective prevention measures, aid in medical diagnosis and improvement of techniques for the auditory rehabilitation. Objective: To evaluate the audio logical profile of the individuals treated in a service of audio logical diagnosis describing the age, gender, chief complaints and to characterize the audiometric thresholds of individuals second degree, type and configuration. Method: A retrospective study, through analysis of medical records of 217 individuals of both genders in the private sector attended in a Brazilian service of diagnostic audiology between January and June 2009. For the study were analyzed the complaints following the evaluation of tonal audiometry. Results: The main complaints were 110 (50.7%) individuals reported tinnitus, 48 (22.1%) dizziness, and 116 (53.4%) dysacusis. The audio logical profile of the individuals was characterized by 36.4% of individuals with normal hearing, 45.6% with dysacusis bilateral and unilateral 18%. When considering both groups with dysacusis there was predominance of the sensory neuro type and of mild grade. Conclusion: The main complaints founded were tinnitus, dizziness, and dysacusis. The Audiometry showed the predominance of bilateral dysacusis of type sensory neuro and of mild grade for the study constituted by adults and seniors individuals attended in the sector.
|
|
|
INTRODUCTION
According to the estimative of the World Health Organization, about 25 millions of the individuals or 4, 7% of the global population presents hearing loss (1). The hearing loss can be recognized already in a child' birth or to be acquired during the life. However, several of these occurrences can be avoided or softened through preventive actions and health promotion (2).
In Brazil, that is considered an emergent country, it is observed a gradual increase with the expectative of individuals' life and consequently the population aging (3, 4). Actually, the life expectative in our country is 72,7 years, according to the Social Indicators Synthesis' data, exposed by Brazilian Institute of Geography and Statistic (5). A phenomenon that results in changes on the population profile, and chronic degenerative diseases of the aging get an emphasis as cardio vascular alterations, diabetes, and hearing loss (2, 3).
The presbycusis as a biological phenomenon that nobody can escape, normally it begins from 20/30 years old and it can render socially uncomfortable about 40/50 years, it is the third affection more common in senior individuals (6, 7).
The auditory system is one of the most important to the development of the process and maintenance of the oral communication and of the quality of life. A failure in this system incites damages and a weak hearing loss can bring problems in the communication (8). Therefore, an audiology diagnosis concomitant to the premature intervention in the dysacusis cases is fundamental to soften such derangements.
In this way, the survey audiological profile becomes an important epidemiological tool to the definition of news health politics, effective measures of prevention, medical diagnosis assistance and consequently technical' upgrading to the auditory rehabilitation (9, 10).
This work aimed evaluate the audiological profile of the individuals treated in a private service of audiological diagnosis describing the age, gender, main complaints and to characterize the audiometric thresholds of individuals second degree, type and configuration.
METHOD
The enchiridion data of 217 individuals were collected of both sexes treated in the private sector of the Audiology Center in São Paulo city, in the period between January and June 2009, before to be conducted by an otorhinolaryngologist doctor.
In this study were not included the enchiridion of individuals with intellectual disability or associates syndromes.
Procedures
The following audiological enchiridion data were collected:
1. Age; sex; Tinnitus complaint, dizziness, or dysacusis collected of the initial interview.
2. Auditory thresholds by aerial via of the frequencies of the 250; 500; 1000; 2000; 3000; 4000; 6000 and 8000 Hz.
3. Auditory thresholds by osseous via, for research of the frequencies of the 500; 1000; 2000; 3000; 4000 Hz.
The auditory thresholds researched was performed in a cabin treated acoustically using the Itera II Audiometer of the GN Otometrics mark with headphones TDH-39 model calibrated in 1 September 2008.
The SILMAN & SILVERMAN'S classification was considered for the analysis of hearing loss type (1997).
In order to the auditory' classification the Biap (1997) table was used, in which it considers the aerial via auditory thresholds average for pure tones of the frequencies of 500, 1.000, 2.000 and 4.000 Hz, adapted with a denomination utilized by LLOYD and KAPLAN (1978).
The thresholds' configuration for hearing loss was based in the audiometric configuration (SILMAN and SILVERMAN, 1997 - adapted of Carhart, 1945 and LLOYD and KAPLAN 1978) categorizing it in: an ascendant, a horizontal, a descendant: a weak, an accentuated or in a ramp, "U," an upside down "U" or Notch.
Statistical Analysis
The qualitative variables related to the sample characterization, complaints were estimated through de percentage of occurrence of its categories, and the confidence intermissions constituted in 95% (11). The age and the sex were calculated by descriptive statistics with confidence intermissions to the average. In the bilateral dysacusis group was utilized the kappa statistic in order to evaluate the results' concordance of the two ears (12).
RESULTS
Between January and June 2009 were evaluated 217 (100%) adults and seniors individuals being 94 (43,3%) of the male sex and 123 (56,7%) of the female sex with the age average of 54,3 years (a pattern deviation of 17,8 years; minimum of 18 and maximum of 103).
Presented complaints analysis
In the attended individuals enchiridion were noticed the presence of one or more complaints being the mains noticed in 110 (50,7%) individuals that presented Tinnitus complaint, 48 (22,1%) of dizziness and 116 (53,4%) with dysacusis.
Audiological profile analysis
By considering the analysis of the hearing degree of the studied individuals, taking into account the Biap (1997) classification adapted of LLOYD & KAPLAN (1978), it was noticed that 79 (36,4%) individuals presented the average of the auditory thresholds within the normality. Of these individuals, 39 (18%) obtained unilateral dysacusis and 99 (45,6%) bilateral dysacusis, according to the represented values in the Figure 1.
In the unilateral and bilateral dysacusis group were analyzed the type, degree and the audiometric configuration.
This study analyzed the audiometric configuration of the Normal group, in order to verify possible auditory alterations in the adjacent frequencies to the average formers frequencies.
Analysis of the group with auditory thresholds within the normality.
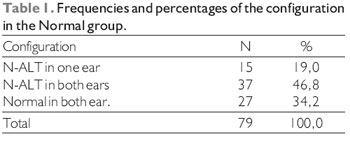
The auditory thresholds' configuration of the normal group was evaluated due to some individuals presenting the average of the auditory thresholds within the normality (auditory thresholds average of the frequencies of 500, 1.000, 2.000, and 4.000Hz) and unsettled thresholds in one or more frequencies evaluated. For the study, it was utilized the "N-ALT" criteria, in other words, normal without alteration, grouping the configurations found as an ascendant, weak descendant, an accentuated descendant in a ramp, notch, in "U" and in upside down "U".
The analysis considered N-ALT in one ear, N-ALT in both ears or normal in both ears, in other words, the auditory thresholds tested within the normality (Table 1).
Analysis of the group with unilateral dysacusis
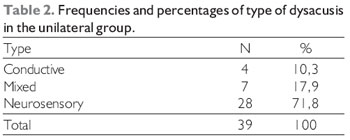
The frequencies and percentages were presented considering the analysis separated of type and dysacusis degree. In this study, it was noticed the presence of the alteration, however without assign which is the affected ear.
Concerning the dysacusis type, 4 (10,3%) individuals presented a Conductive, 7 (17,9%) a Mixed and, 28 (71,8%) a Neurosensory (Table 2).
Among the individuals with dysacusis, 20 (51,3%) of them presented a weak degree, 6 a moderate, 2(5,1%) a moderately severe , 5(12,8%) a severe and, 6 (15,4%) with an intense degree.
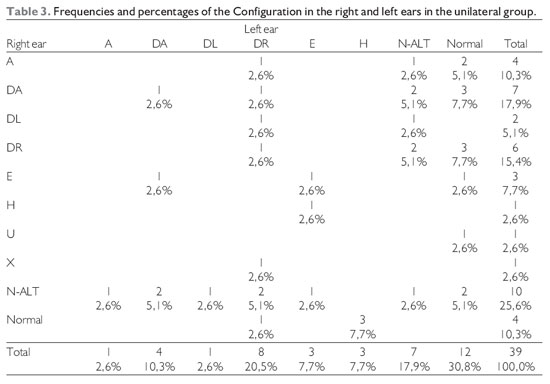
The auditory thresholds' configuration was observed in both ears and the frequency and percentage of the data interlacement presented in both ears can be noticed in the Table 3.
Analysis of the group with bilateral dysacusis.
The distribution of the type, degree, and auditory thresholds configuration considered the found results in both ears.
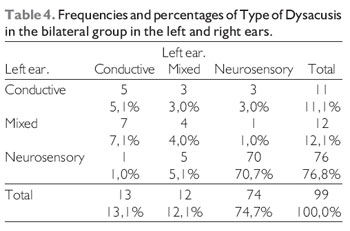
The distribution of the dysacusis type in the bilateral group in the right and lest ears demonstrated the possibility of the individuals presented identical types or different between the ears, as a example, 5 (5.1%) of the individuals have conductive type dysacusis in both ears. Three (3%) have a conductive in the right ear and mixed in the left and, 3 (3%) have a conductive type in the right ear and Neurosensory in the left. The observed value of the kappa statistic was 0,49 (standard error=0,07), considering a moderate concordance of the findings of the measures in both ears (Table 4).
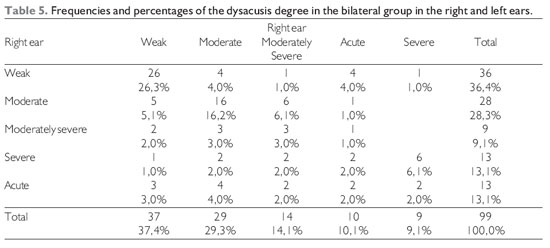
The bilateral dysacusis degree was interpreted likewise the type, however the kappa statistic value was 0,38 (standard error of 0,06) pointing out a concordance almost moderate (Table 5).
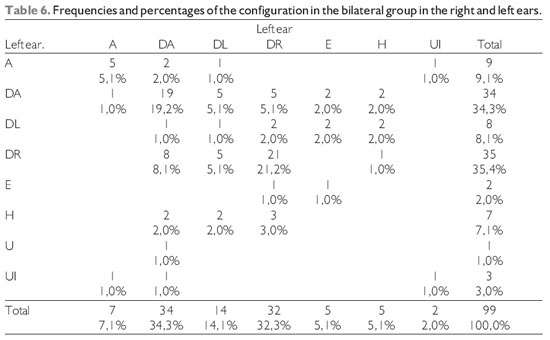
In the thresholds' configuration analysis to the category of bilateral dysacusis, in the kappa statistic calculation were gathered the categories related to the descendant configuration (weak descendant, accentuated and in a ramp) and the "U" configuration (in "U" and in upside down "U"). Therefore, it is find the kappa statistic value equal to 0,03 (standard error=0,10) that indicates weak concordance between the results in both ears (Table 6).
DISCUSSION
The present study noticed the female sex predominance in the studied sample, affording to consider that possibly the women presented major availability to search medical assistance (13) or major interest in the treatment (15). However, this data becomes insufficient to characterize the hearing loss prevalence.
Despite several studies point the impact originated of the hearing loss in the quality of life there is a larger diversity in the prevalence findings of the hearing loss in adult individuals by considering the variables of age, race, exposition to noises and also diseases associated or tabagism (1,2,3,4,5,6,7, and 8) in the studied groups.
This study does not reflect the general population prevalence once it was characterized the audiological profile only of the patients that looked for medical evaluation, and needed it audition evaluation.
Patients that looked for an exams service and audiological diagnosis, frequently presented other otological complaints associated to the complaint of dysacusis as Tinnitus (13,15), dizziness (14,15) and visual alteration (15). Our study noticed like the main complaints, initially dysacusis followed by Tinnitus and dizziness.
Despite not to be main complaints, in our study we have noticed anxiety complaints, hypertension, or diabetes mellitus as factors that induced the individuals to do audiological evaluation.
BARROS et al. (13) related a major number of cases with neurosensory hearing loss and with a weak degree in bilateral alterations. In the research, there was convergence of the results finding a major number of individuals with a neurosensory type dysacusis and weak degree (13, 16) to the bilateral group, with the study cited previously, as well as to the group with unilateral dysacusis.
In the auditory thresholds' individuals' group within the normality, 19% of the individuals presented unilateral alteration in high frequencies and 46% bilateral alterations in high frequencies according to the AGRAWAL et al (8) study that describes to have found bilateral alteration predominance in high frequencies.
With the present study, by considering only the auditory thresholds average of 500, 1000, 2000, and 4000 Hz within the auditory thresholds of normality for intensity equals or below to 25dBNA, it faced the risk of detection loss of a subgroup of individuals with alteration in high frequencies. Therefore, it is proposed the need of observation of frequencies adjacent in the young adults individuals' exams for a effective prevention.
CONCLUSION
The study noticed that the first auditory complaints pointed by individuals were dysacusis, following by Tinnitus and dizziness. The audiological profile of the individuals was characterized for: 36,4% of individuals with normal hearing, 45,6% with bilateral dysacusis and 18% unilateral. By considering both groups, there was the type neurosensory predominance of weak degree.
BIBLIOGRAPHICAL REFERENCES
1. Mathers CD, Smith A, Concha M. Global Burden of hearing loss in the year 2000.2000. Disponível em: www.who.int/entity/healthinfo/statistics/ bod_hearingloss.pdf.
2.Brasil. Ministério da Saúde. Prevalência da perda auditiva. Disponível em: portal.saude.gov.br/portal/arquivos/pdf/manual2.pdf.
3. Marques ACO, Koslowski L, Marques JM. Reabilitação no idoso. Rev Bras Otorrinolaringol. 2004, 70(1):806-11.
4. Teixeira AR, Almeida LG, Jotd GP, De Barba MC. Qualidade de vida de adultos e idosos pós- adaptação de próteses auditivas. Rev Soc Bras Fonoaudiol. 2008, 13(4):357-61.
5.Instituto brasileiro de Geografia e Estatística. Indicadores. 2008. Disponível em: http://www.ibge.gov.br/home/estatistica/populacao/condicaodevida/ indicadoresminimos /sinteseindicsociais2008/default.shtm.
6.Bilton T, Ramos LR, Ebel S, Teixeira LS, Tega LP. Prevalência da deficiência auditiva em uma população idosa. O mundo da saúde. 1997, 21(4):218-25.
7. Portmann M, Portmann C. Tratado de Audiometria Clínica. 6ª ed. São Paulo: Roca; 1993.
8. Agrawal Y, Platz EA, Niparko JK. Prevalence of hearing loss and differences by demographic characteristics among US adults. Arch Intern Med. 2008, 168(14):1522-30.
9. Lima-Costa MF, Veras R. Saúde pública e envelhecimento. Cad Saúde Pública. 2003, 19(3):700-1.
10. Lima e Costa MFF, Guerra HL, Barreto SM, Guimarães RM. Diagnóstico da situação de saúde da população idosa brasileira: um estudo da mortalidade e das internações hospitalares públicas. Inf Epidemiol Sus. 2000, 9(1):43-50.
11 Bussab WO, Morettin PA. Estatística Básica, 5a ed. São Paulo: Editora Saraiva; 2002.
12. Sim J, Wright CC. The Kappa Statistic in Reliability Studies: Use, Interpretation and Sample Size Requirements. Physical Therapy. 2005, 85(3):257-68.
13. Coelho CCB, Sanchez TG, Bento RF. Características do zumbido em pacientes atendidos em serviço de referência. Arq Int Otorrinolaringol. 2004, 8(3):216- 24.
14. Moreira DA, Bohlsen YA, Momenshon-Santos TM, Cherubini AA. Estudo do Handicap em pacientes com queixa de Tontura, associada ou não ao sintoma de Zumbido. Arq Int Otorrinoringol. 2006, 10(4):270-7.
15. Morimoto WTM, Medina NH, Guardado NA, Lima MHA, Pinto AMM, Magnunsson IM. Avaliação visual e auditiva em adultos e idosos na atenção básica. 2006. Disponível em: http://www.cve.saude.sp.gov.br/agencia/bepa30_aval.htm.
16. Mattos LC, Veras RP. A prevalência da perda auditiva em uma população de idosos da cidade do Rio de Janeiro: um estudo seccional. Rev Bras Otorrinolaringol. 2007, 73(5):654-9.
1. PhD in Science by the University of São Paulo's Medicine School. Speech therapy.
2. Speech therapist with Improvement in Cochlear Implant by the Hospital das Clínicas of the University of São Paulo's Medicine School.
3. Student of the Advance Course of Clinic Audiology at Hospital das Clínicas of the University of São Paulo's Medicine School.
Instituition: Center of Audiology São Paulo. São Paulo / SP - Brazil. Mail Adress: Isabela de Souza Jardim - 352, Teodoro Sampaio, St. Cj 151 -São Paulo /SP - Brazil - ZIP: 05406-000 - Phone: (+55 51) 3062-9328 - E-mail: isasjardim@gmail.com. Article received on 11 December 2009. Approved on 24 January 2010.
|
|
 |
|
|
