 |
705 |
|
| Year: 2010 Vol. 14 Num. 3 - Jul/Set - (8º)
|
|
 |
| Section:
Original Article
|
|
|
|
|
| Vocal Self Assessment Questionnaire: Epidemological Control Tool of the Ocupational Dysphonic Syndrome in Professors |
|
| Author(s): |
| Sandra Irene Cubas de Almeida1, Paulo Pontes2, Marco Antonio Bussacos3, Luciano Neves4, Fabiana Zambon5.
|
|
|
| Key words: |
| dysphonia, occupational medicine, occupational risks, worker health, research. |
|
|
 |
| Abstract: |
Introduction: The dysphonic syndrome is an occupational disease of high prevalence in the professor population. Objective: In order to broach preventively the vocal aggression, it was tried to standardize a self assessment questionnaire to professors of all educational level, including beyond the clinical symptoms also the factors of the work organization. Method: It was performed a study of transversal cut in 328 professors of 4 educational institutions of the northern of São Paulo, which it was applied a self assessment questionnaire elaborated by TRipartite Commission of Standardization for Professional Voice. Results: It was determined the prevalence of clinical symptoms that compound the dysphonic syndrome, as well as it was delineate the work organization and the quality of life of this population. Conclusion: The questionnaire applied was showed itself satisfactory en the description and elaboration of parameters with the aim of to implement preventive programs to populations exposed to professional overload of the voice use. Case study.
|
|
|
INTRODUCTION
Self-assessment of risk is a vocal initial non-invasive procedure, part of the arsenal of diagnostic methodology, designed to be applied to control epidemic and individual, with the goal of early detection and prevention of occupational dysphonic syndrome.
Dysphonic occupational syndrome (ODS) refers to the set of signs and symptoms caused by or triggered dysphonic voice use in professional activities that may be related to other causes such individual predisposition and environmental factors. (1)
The pre-pathogenic can lead to permanent alteration of the vocal emission by establishing laryngopathies and in such cases, called laryngopathies related to work.
Signs and symptoms of dysphonic syndrome are: pain or irritation in the throat, and foreign body sensation, neck pain, need for throat clearing and hoarseness and preventive medical measures that may present themselves effective when it can track all quoted earlier. So the dysphonic syndrome is a warning signal in which the measures and procedures specific to wide variation according to individual needs, should be initiated aimed at preventing laryngopathy.
Clinical research of signs / symptoms is, by international consensus, recommended by the European Laryngological Society, one of the actions required minimum basic research in any diagnostic action and / or therapy on the speech organs. (2)
The basic principles to be followed in preparing a vocal self-evaluation are:
1. Consider that vocal function is multidimensional.
2. Obtain records that allow conclusions to the meta-analysis.
3. Not exclude other procedures that may be necessary, but precede them.
Several studies have been published in order to obtain the prevalence of dysphonia in teachers using self-assessment questionnaires or not associated with clinical examinations. The value of this prevalence ranged from 0.8 to 34% (3,4).
From 1998 there was an increase in prevalence to 70%.
In 1998, an Australian group teachers evaluated and defined by drafting questionnaires the prevalence of clinical complaints vocals in this population (4).
The aim of this study is to validate a self-evaluation directed the vocal category of teachers of all levels of education for tracking of dysphonic symptoms of the syndrome and occupational factors in the organization of work that interfere with the natural history of occupational laryngopathies.
METHOD
We conducted a cross-sectional epidemiologic study of 328 teachers from four teaching institution in the northern region of São Paulo from 2001 to 2002.
These teachers were applied to self-evaluation prepared by the Tripartite Commission on Standardization of Voice Training (5).
The criteria for the elaboration of self-evaluation were:
1. Define the identification of individuals by sex, age, body maintains.
2. Organization of work in relation to employment with other institutions, levels of education for which he teaches, workload, breaks, number of students per class, the exercise of other professional activities.
3. Clinical symptoms of the syndrome dysphonia.
4. Habits and quality of life.
The application was performed for the class intervals and beginning the same.
Preceding the application, held the spot verification of the conditions and environmental factors, as well as the organization of work detailed in the self-assessment questionnaire.
As part of the method we performed the dissemination of the techniques of vocal hygiene after the implementation of self-evaluation.
Given the objective of validating the self-assessment to define the population profile by indicating the prevalence of symptoms of dysphonic syndrome as well as determining the characteristics of the population that can act as risk factors in the evolution of the disease, the questionnaire should meet the following criteria:
1. Easy to understand the questions and answers.
2. Time taken to answer the entire set.
3. Suitability of format for statistical analysis.
4. Evaluation of the individual on the desktop and in your organization.
5. Tracking the symptoms of the syndrome as a manifestation of occupational dysphonia pre-pathogenic or pathogenesis early in the installation of an occupational laryngopathy organic or functional disabling.
6. Consensus social approval of the members of the Tripartite Commission.
Questionnaires were administered to all teachers who were in the staff room during the period preceding the start of classes and after the express informed consent of the participant.
After approval by the Medical Ethics Committee of UNIFESP and signing of Informed Consent, teachers and the institution received guidance on vocal hygiene, prevention and control of medical risk related laryngopathy work and questionnaires were administered by medical staff of MTE (Ministério Labor and Employment), UNIFESP (Federal University of São Paulo) accompanied by representatives of the Teachers' Union of São Paulo (Sinpro-SP), for their safety and health of the institution and members of the Internal Commission for Accident Prevention (CIPA ).
The operationalization of the method occurred in situ by applying the self-assessment, the forensic verification of compliance with regulatory standards that establish medical control, control of environmental risks and ergonomic conditions and organization of work (6).
The database was created in Excel and the analysis used the software SAS / SAT 9:12 version on statistical analysis FUNDACENTRO.
RESULTS
328 questionnaires were administered self-assessment for teachers of four institutions of higher education located in the northern region of Sao Paulo.
Self-evaluation has been prepared and divided into four parts:
1. Identification.
2. Organization of work.
3. Clinical symptoms.
4. Habits and quality of life.
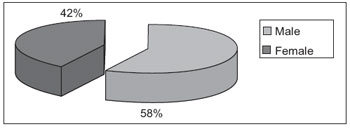 Graphic 1. Prevalence of gender.
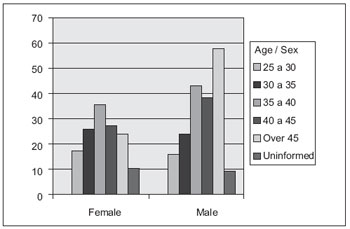 Graphic 2. Distribution of age groups between genders.
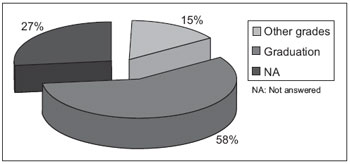 Graphic 3. Prevalence of linkages with other institutions.
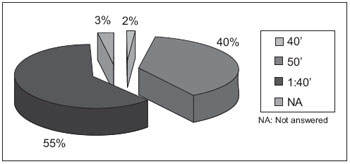 Graphic 4. Prevalence of the duration of the lessons.
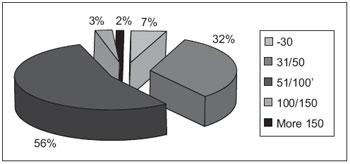 Graphic 5. Prevalence of students per classroom.
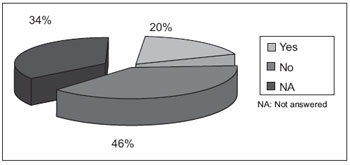
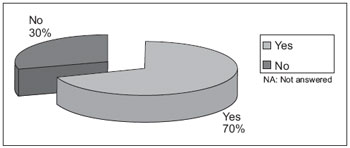 Graphic 6. Prevalence of clinical symptoms pain or irritation in the throat.
 Graphic 7. Prevalence day period in which there is a clinical symptom pain or irritation in the throat.
DISCUSSION
When we started the study on the prevalence and evolution of the syndrome occupational dysphonia in teachers needed to develop a methodological approach to show us the characteristics of this population and provide concrete evidence that we might propose effective control measures.
Therefore, since the syndrome occupational dysphonia a set of signs and symptoms early in the establishment of an occupational laryngopathy, the initial multidimensional approach gives us criteria for the prevention of pathogenic consequences that culminate with the exclusion of individuals to their professional environment.
One of the first findings that we had was the discrepancy between the legal requirements and the actions performed in the institutions, ie a decoupling between the control run and the proposed medical and occupational risk as vocal advocates legislation through the principles of Regulatory Standard 7 (7) .
From this work in the institutions, programs for the control of occupational health began to consider measures aimed at health risks Syndrome dysphonia.
The review of the literature (3,4,7) have shown that this is a universal concern which is the approach of considering the syndrome Dysphonic manifestation of individual and aspects of their vocal production.
One of the best-known works is about evaluating the Vocal Handicap Index which has been studied and validated in languages other than English.
Through the Graphics, we can define characteristics of the population health and proposes actions for the subjects tested, we can add to control the clinical data and follow them prospectively.
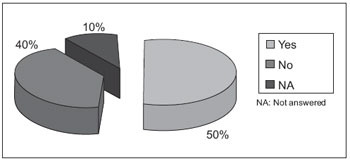
The graphs show that this population of academics there is a predominance of men (Graphic 1) in patients aged over 35 years (Graphic 2) with dedication to higher education (Graphic 3).Regarding the organization of work, the predominant classes of more than 100 minutes (Graphic 4) and the number of students per class is more than 51 for most (Graphic 5). The symptom of pain or irritation in the throat occurs in 70% being more frequent at night (Graphics 6 and 7). Feeling of foreign body is reported in 41% (Graphic 8). The need of throat and neck pain occurs in 54% (Graphics 9 and 10). Hoarseness was reported by 31% (Graphic 11). Smoking was stated by 16% (Graphic 11) and some intake of alcohol and prescription drugs continuously for 20% (Graphic 12 and 13). Sporting activity is practiced by 50% evaluated.
So the diversity is evident in the prevalence of individual symptoms that comprise the SDO which justifies the different values of the occurrence of dysphonia in teachers presented in the literature.
Self-assessment has its own characteristics targeted to local needs and aims to provide evidence of epidemiological control.
Introduction of new questions to the text was always preceded by discussions with the Tripartite Commission and resulted from the difficulties and observations that we had at work and its practical application, always aiming to maintain objectivity and simplicity of understanding with the least expenditure of time for your application.
Since it is a basic action of health, must be used by the occupational physician who maintains the epidemiological control population and to the otolaryngologist is a non-restrictive element initial indication of the more complex procedures.
Through the graphs we can define the characteristics of population health and proposes actions for the individuals tested, we can add to control the clinical data and follow them prospectively.
Based on these findings we can say that from a self-evaluation should make proposals that act to reduce the prevalence of SDO thus preventing the emergence of laryngopathies disabling.
The development of self-assessment with technical and social consensus proved to be adequate as well as being an inexpensive procedure is noninvasive and also abolishes techniques that may become discriminatory.
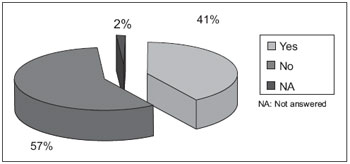 Graphic 8. Prevalence of symptom foreign body sensation in the throat.
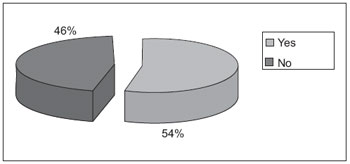 Graphic 9. Prevalence of symptom throat clearing.
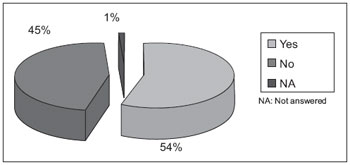 Graphic 10. Prevalence of neck symptoms.
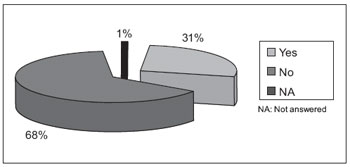 Graphic 11. Prevalence of hoarseness.
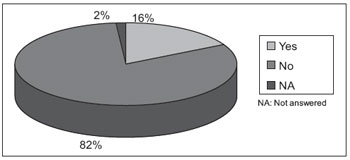 Graphic 12. Prevalence of smoking.
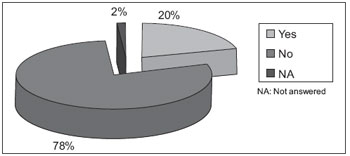 Graphic 13. Prevalence of alcohol.
 Graphic 14. Prevalence of drug use.
 Graphic 15. Prevalence of the practice of sports activities.
CONCLUSION
The self-assessment questionnaire for teachers proposed by the Tripartite Commission for Standardization of Professional Voice was satisfactory to provide the prevalence of parameters that allow epidemiological analysis of occupational dysphonia in teacher's syndrome.
BIBLIOGRAPHICAL REFERENCES
1. Leavell H & Clark EG. Medicina Preventiva. McGrawHill do Brasil, São Paulo, 1976.
2. Dejonckere P H et al. A basic protocol for functional assesment of voice pathology especially for investigating the efficacy of (phonosurgicals) treatments and evaluating new asesment techniques. Eur Arch Otorhinolaryngol. 2001, 258:77-82.
3. Smith E et al. Frequency and effects of teachers voice problems. J Voice. 1997, 2:81-87.
4. Russel A, Oates J, Greenwood K. Prevalence of voice problems in teachers. J Voice. 1998, 12:467-479.
5. Ministério do Trabalho e Emprego (2002) Comissão Tripartite de Normatização para a Voz Profissional. Questionário de auto-avaliação para professores. Imprensa Oficial do Estado. 11 páginas.
6. Ministério do Trabalho e Emprego. Portaria 3214.
7. Calas M et al. La pathologie vocale chez l'enseignant. Rev Laryngol. 1989, 110:397-406.
1 Doctor of Medicine. Head of the Labour Relations MTE-Management North / SP.
2 Professor, Department of Otolaryngology and Human Communication Disorders, UNIFESP.
3 Researcher Fundacentro.
4 Master in Otorhinolaryngology at UNIFESP Otorrinolaringologia.Douturando.
5 SLP. Speech Therapist Sinpro / SP.
Institution: Ministry of Labor - Management North. São Paulo / SP - Brazil. Mail address: Sandra Irene Cubas de Almeida - Av General Ataliba Leonel, 2764 - Parada Inglesa-Sao Paulo / SP - Brazil - Zip code: 02242-000 - Telephone: (+55 11) 2973-8927 - E-mail: sandra.almeida@mte.gov.br
Article received on April 8, 2010. Article accepted on 29 May 2010.
|
|
 |
|
|
