 |
732 |
|
| Year: 2010 Vol. 14 Num. 4 - Out/Dez - (17º)
|
|
 |
|
|
| Endoscopic Escalated Resection to Extensive Amyloidosis of the Upper Aero-digestive Tract: a Feasible and Effective Alternative |
|
| Author(s): |
| Thiago Chianca Ferreira1, Carlos Eduardo Fernandes Soares de Melo1,Fernando Martinez Belentani2, Mayko Soares Maia2, Romualdo Suzano Louzeiro Tiago3.
|
|
|
| Key words: |
| Amyloidosis, Larynx, Microsurgery. |
|
|
 |
| Abstract: |
Introduction: Localized amyloidosis is a rare disease characterized by extracellular deposition of proteins that can occur in various regions of the body. The larynx is the most common site of disease in head and neck. Objective: We present a literature review and the case of a patient with extensive amyloidosis in the upper aero-digestive tract, whose resection was performed in four steps. Case Report: SMS, 28 years, 4 months ago dysphonia. Complementary exams showed large lesions in supraglottic that was removed in four stages by microlaryngoscopy. Final Comments: microlaryngoscopy tiered approach was effective and safe resection of lesions in amyloidosis large.
|
|
|
INTRODUCTION
Amyloidosis is a disease characterized by extracellular deposition of proteins in various body regions (1.2). It may be localized or systemic, inherited or acquired (3). Virchow was the first to use the term because of his amyloidosis type amyloid reaction when treated with sulfuric acid. Laryngeal localized disease was viewed first by NEUMANN and BORROE on examinations of cadavers (2.4).
Among the benign tumors of the larynx, amyloidosis accounts for only 1% of cases. However, it is the most common site of amyloid disease located in the head and neck. The most common symptom is dysphonia, may also be present with dyspnea and dysphagia (4).
The histopathology is characterized by greenish birefringent when stained by Congo red.
The recommended treatment is surgical excision of the lesion from microlaryngoscopy. The technique can be used with a scalpel, CO2 laser or external lateral approach in extensive lesions (1,3,5).
Our goal is to report the outcome of a patient with extensive amyloidosis in the upper aero-digestive tract, whose resection was performed incrementally in four stages.
CASE REPORT
SMS, 28, was referred with complaints of dysphonia with 4 months of evolution. She denied dyspnea or dysphagia. The patient had a muffled voice, and with little projection. The fibronasopharyngolaryngoscopy showed a yellowish mass lesion in the vestibular fold aryepiglottic ligament and the right side, limited to the supraglottic region (Figure 1). In computed tomography (CT) was shown a heterogeneous mass lesion with irregular borders, extending to the vestibular fold and the right ventricle (Figure 2). Biopsy stained by Congo red and examined in the polarizing microscopy (green birefringence) confirmed that it was laryngeal amyloidosis. The patient was referred for clinical investigation for the presence of systemic amyloidosis with appropriate examinations and complete blood count, coagulation, AST, ALT, alkaline phosphatase, total bilirubin and fractions, urea, creatinine, uric acid, blood glucose, serum calcium, total protein and lipoproteins, CRP, ESR, rheumatologic tests, electrocardiogram, chest radiography and abdominal ultrasound and all were negative.
He underwent surgical resection for microlaryngoscopy. The resection technique was spread over four stages with electric cautery for resection of the laryngeal lesion. Between the first and last step, the interval was about 2 years.
In the first procedure was performed to resect the lesion located in the aryepiglottic fold and most of the lesion of the right vestibular fold, thus sparing the posterior region of the larynx in order to avoid stenosis in this region. The residual lesion in the posterior region of the larynx, located above arytenoid was resected in the second procedure. In the third stage, withdrew from the lesion located in the posterior third of the right vestibular fold.
Between the third and fourth intervention, the lesion was observed at the base of the tongue to the left (Figure 3), which was removed in the fourth procedure, with the histopathologic diagnosis of amyloidosis in the base language. Therefore, this lesion was a second focus of amyloidosis in the upper aero-digestive tract.
In the fourth and final procedure was resected focus of amyloidosis localized in the anterior third of the vestibular fold the right side (Figure 4), besides the previously described lesion in the tongue base. The patient has been followed with periodic examinations laryngoscopic without symptoms or signs of disease recurrence (Figure 5).
 Figure 1. Telelaryngoscopy where it can be observed lesion located in the supraglottic (aryepiglottic and vestibular folds) on the right side and with obstruction of approximately 60-70% of laryngeal adit.
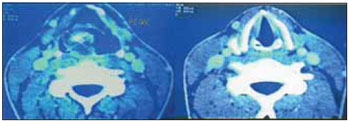 Figure 2. Computed tomography of the cervical, supra-glottis, where it can be observed lesion with soft tissue density in the right aryepiglottic fold (left) no lesion in the glottis (right).
DISCUSSION
Amyloidosis is a rare disease characterized by extracellular deposition of proteins and of unknown etiology. Biochemically, it can present itself in many different ways, the most important being the AL, AA and AB. The AL type is derived from plasma cells containing immunoglobulin light chains kappa and lambda, may be localized or systemic, and is associated with multiple myeloma. The AA is comprised of the serum amyloid A, is a systemic amyloidosis, and is associated with chronic inflammatory diseases. Type AB is associated with Alzheimer's disease cases and occasional family (2).
The preferred site for laryngeal amyloidosis are the aryepiglottic and vestibular folds, and the most frequent symptom is dysphonia (1,3,6). Rarely, the laryngeal amyloidosis composed manifestation of systemic disease, and almost always restricted to laryngeal disease (3,4). The patient presented initially with complaints of dysphonia and was found a lesion that affected aryepiglottic, vestibular folds and the laryngeal ventricle on the right, without compromising the vocal folds. Systemic disease was excluded after specific investigation.
The amyloid lesion should be removed surgically, and whenever possible in a conservative manner (1,2,3,5,6). Other treatments such as corticosteroids, radiotherapy and chemotherapy have proven ineffective (5). For extensive disease or with multiple relapses, KENNEDY and PATEL used the technique of external lateral approach, showing good results in both cases underwent surgical treatment (4). However, the external approach for resection of extensive laryngeal amyloidosis is related to the neck scar and the degree of morbidity (dysphagia and dysphonia). The patient reported he was approached by microlaryngoscopy, with the removal of the lesion was performed with electrocautery in four steps order to avoid extensive resection and possible formation of adhesions and laryngeal stenosis. The result was satisfactory, because the patient showed complete remission of symptoms and the lesion was completely resected.
We emphasize that this approach is possible when we have a cooperative patient, in whom we have confidence that the monitoring will be done satisfactorily.
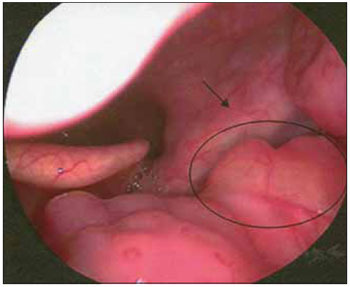 Figure 3. Telelaryngoscopy where injury can be observed at the base of the tongue, left side, yellowish.
 Figure 4. Telelaryngoscopy where residual lesion can be seen above, dried in the last procedure.
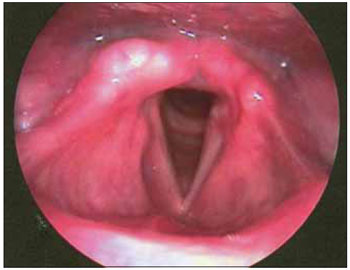 Figure 5. Telelaryngoscopy control after the fourth procedure, no signs of injury in the supraglottic (arypiglottic and vestibular folds).
CONCLUSION
Amyloidosis is a rare disease that the otolaryngologist should consider as a differential diagnosis in laryngeal lesions. When diagnosed, should be ruled out associated systemic disease.Surgical treatment of extensive lesions can be performed from microlaryngoscopy in two or more steps. This approach proved effective and safe in treating a patient with localized amyloidosis in the upper aero-digestive tract (supraglottic region and base of tongue).
BIBLIOGRAPHIC REFERENCES
1. Dedo H, Izdebski K. Laryngeal amyloidosis in 10 patients. Laryngoscope. 2004, 114:1742-6.
2. Alaani A, Warfield AT, Pracy JP. Management of laryngeal amyloidosis. J Laryngol Otol. 2004, 118:279-83.
3. Penner C, Muller S. Head and neck amyloidosis: a clinicopathologic study of 15 cases. Oral Oncology. 2006, 42:421-9.
4. Kennedy TL, Patel NM. Surgical management of localized amyloidosis. Laryngoscope. 2000, 110:918-23.
5. Avitia S, Hamilton JS, Osborne RF. Surgical rehabilitation for primary laryngeal amyloidosis. Ear Nose Throat J. 2007, 86:206-8.
6. Thompson LDR, Deringer GA, Wenig BM. Amyloidosis of the larynx: a clinicopathologic study of 11 cases. Mod Pathol. 2000, 13:528-35.
1 Graduation. Resident.
2 ENT. Former Resident.
3 Doctor of Science at the Graduate Program in Otolaryngology and Head and Neck Surgery, UNIFESP. Attending Physician.
Institution: Department of Otorhinolaryngology, Hospital do Servidor Publico Municipal de São Paulo (HSPM). São Paulo / SP - Brazil. Mail Adress: Thiago Chianca Ferreira - Rua Francisco Jose Longo, 210 - Apto. 72 - Finca English - São Paulo / SP - Brazil - Zip code: 04140-060 - Telephone: (+55 11) 7691-3738 - E-mail: thiagocferreira@yahoo.com.br
Article received on 12 May 2009. Approved on July 27, 2009.
|
|
 |
|
|
