|
738 |
|
| Year: 2011 Vol. 15 Num. 1 - Jan/Mar - (5º)
|
|
 |
| Section:
Original Article
|
|
|
|
|
| Comparison of Indicators of Risk of Deafness in Newborns Studied in the Years 1995 and 2005 |
|
| Author(s): |
| Monique Kelly Duarte Lopes1, Teresa Maria Momensohn Santos2.
|
|
|
| Key words: |
| deafness, disease, newborn. |
|
|
 |
| Abstract: |
Introduction: The data submitted by the Center of Epidemiological Surveillance of the State of São Paulo indicates the number of children affected by infecto-contagious diseases increases yearly. Some of these diseases are considered to be of risk for hearing. Objective: Check and compare the occurrence of risk indicators of the Hearing Loss during the interval of 10 years in a maternity of São Paulo. Method: Quantitative and retrospective study carried out from the research and review of data of registers supplied by a maternity of the city of São Paulo. We surveyed the registers of babies who were born from January through December of the years of 1995 (n=2.077) and 2005 (n=5.129), including those who had risk indicators for deafness and prematurity, low weight and asphyxia, besides having a diagnosis confirmed or suspicion of infecto-contagious diseases of group TORSCH-A. Results: We reviewed reports of 565 children born in 1995, and 1047 born in 2005. Among the risk indicators of deafness, we noticed a significant difference for the indicator of prematurity and asphyxia and there was no significant difference for the low weight indicator. The risk indicators of prematurity, low weight and asphyxia were more frequent than Toxoplasmosis, Syphilis and HIV+. The children born in 1995 tended to have a higher number of risk indicators and/or diseases than those born in 2005 (p<0.001). Conclusion: The major incidence of indicators in 1995 appoints an improvement to health that diminishes the index of newborns with risk of deafness along 10 years.
|
|
|
INTRODUCTION
The process of acquisition and development of speech and language has a strict relationship with hearing. The identification of the auditory changes right in the first months of life of the baby allows the occurrence of intervention still in the critical period ideal for stimulation of language and hearing, which enables the development of the capacity to receive, recognize, identify and discriminate the sounds around them (1, 2).
Therefore, the concern and the recommendations on the phonoaudiological intervention, as a way to prevent and/or mitigate the consequences of the lack of sound stimulation due to the hearing loss have given rise do many researches (3) indicating that in Brazil 65% of the cases of deafness in childhood result from problems acquired in the prenatal and/or postnatal period, while 4% are a consequence of hereditary causes (4).
It is known that 2-4:100 newborns admitted in the Intensive Care Unit (ICU) have bilateral hearing loss (5), which may be caused by congenital infections for mother to infant transmission. These have deserved attention for some decades due to the concern with the sequels and damages they cause to hearing (6).
In 1974, the infectionist NAHMIAS (7), already concerned with the sequels of infecto-contagious diseases for mother to infant transmission and aiming to draw attention from the physicians for the existence of this group of congenital infections with similar characteristics, created the acronym TORCH (Toxoplasmosis, Congenital Rubella, Cytomegalovirus and Herpes). In 1982, JCIH added to the acronym TORCH the letter S, indicating Congenital Syphilis and currently it is known as TORSCH-A, for it received another addition of letter A, from AIDS.
Nevertheless, even with the concern of some researchers, we still notice the risk indicators present upon birth have not been deemed to be indicators of hearing alteration (8), even after establishment of the relationship between some congenital infections and the hearing loss, as shown by a study on the most frequent infectious agents related to hypacusis, including Cytomegalovirus, Rubella virus, gondii Toxoplasma and Herpes virus (9, 10, 11, 12, 13).
Faced with the data presented we consider the need of epidemiological studies on the occurrence of risk indicators, especially of TORSCH-A group diseases in the population of newborns, because a survey of this nature will allow that actions and programs for promotion of woman's health may be implemented (14, 15).
As well as recommendations with guidance on how to prevent infecto-contagious diseases by mother to infant transmission, by changing in a safe and effective manner the risks to the hearing to their children, in addition to keep close attention to Toxoplasmosis, Herpes and the Cytomegalovirus in the recommended notification category, once these are part of the risk indicators for deafness presented by the JCIH.
Therefore, the objective of this study is to verify and compare the occurrence of risk indicators for hearing loss during the interval of 10 years (1995 and 2005) at a hospital of the city of São Paulo - SP.
METHOD
This research was approved by the Ethics Committee in research of the Hospital Municipal e Maternidade Escola Dr. Mário de Moraes Altenfelder Silva - SP, under the number 39/08, and was qualified as quantitative, retrospective. A secondary data survey and analysis were carried out from the records of books supplied by the Baby Ward of Hospital Municipal e Maternidade Mário de Moraes Altenfelder Silva - SP, popularly known as Maternidade Vila Nova Cachoeirinha.
The sample was composed by secondary available records of the babies born in the maternity, in the period from January through December of the years between 1995 and 2005.
The choice of the 10 years interval of 1995 and 2005 resulted from analysis of the history of actions of the Ministry of Health that were taken in the country for the TORSCH-A group diseases considered to be risk indicators for deafness.
With the loss of some data of the year 1995 it was possible to survey the number of 2077 newborns and for the year of 2005 the value of 5129. After this first survey the analysis of Diagnosis Books analysis was started regarding the years defined, which were submitted to a process of triage. The inclusion criteria adopted were:
- Having risk indicators for Hearing Loss: Prematurity, Low Weight and Asphyxia;
- Having cases confirmed, suspected or exposed of one of the infecto-contagious diseases of TORSCH-A group, appointed by JCIH in 2007.
At the end of this selection 565 newborns were found with risk indicators for Hearing Loss (HL) in 1995, and 1047 newborns with some risk indicator of HL for the year 2005, and such values were taken as the composition of the sample for each year.
Consequently, the study kept on involving the sample analysis of reports of 565 children born in 1995, and 1047 children born in 2005. The following variables were noticed:
- Gender: female or male;
- Weight: in kg;
- Gestational Age: in weeks;
- Prematurity: yes or no;
- Low weight: yes or no;
- Asphyxia: yes or no;
- Consanguinity: yes or no;
- Toxoplasmosis: confirmed, suspect or not;
- Rubella: confirmed, suspect or not;
- Syphilis: confirmed, suspect or not;
- Cytomegalovirus: confirmed, suspect or not;
- Herpes: confirmed, suspect or not;
- HIV: exposed or not.
The other risk indicators described by the JCIH in 1994 and 2007 were disregarded for lack of information in the description of the Hospital Discharge of the individuals.
Besides having been verified whether having low weight or not, the variable Weight was used in the creation of a weight range category: < 1500g, 1500 to 2500g e >2500g, from the numbers referred to in the record book. The data obtained in each year was described in a worksheet of program Microsoft Excel 2003.
In order to compare the distributions of Sex, Weight range and Risk indicators in the years 1995 and 2005 the Chi-Square test (BUSSAB and MORETTIN, 2002) was applied. In the hypothesis tests the significance level was set at p<0.05, and the analysis was carried out with the help of the applications Statistical Package for Social Sciences (SPSS) version 11.0 and Minitab version 15.
RESULTS
When comparing each risk indicator between the two years we noticed the Prematurity had a significant difference between the distribution of the percentages in both years, and the percentage of premature children was higher in 1995 (p<0.001). The risk indicator of Low Weight did not present a significant difference between the percentages of occurrence (p=0.209); the Asphyxia had a significant difference in the percents of both years (p=0.027), and the percent of occurrence in 1995 was higher than that of 2005 (Table 1).
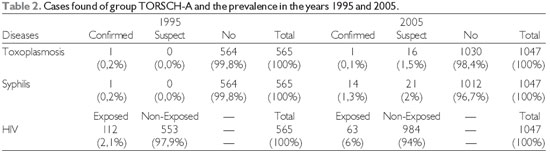
Table 2 describes the distributions of frequencies and percentages of the diseases found in the books analyzed (Toxoplasmosis, Syphilis and HIV) in both years. The children who were not classified in the worksheet as not having confirmed, suspect or exposed cases were considered not to have the disease. In 2005, there were 17 cases (1.6%) confirmed or suspect of Toxoplasmosis and there was a significant difference between the percents of absence of this disease in both years, with a higher occurrence (confirmed or suspect) in 2005 (p=0.008). As regards to syphilis, there was only 1 case confirmed in 1995 (0.2% of all children in this year). In 2005 there were 14 confirmed and 21 suspect cases that correspond to 3.3% of the children born in this year. There was a significant difference between the percents of occurrence of Syphilis in both years (p<0.001) and the higher percent of occurrence was in 2005. For HIV there was a difference between the percents of children exposed to the disease in both years (p<0.001), with the percent of exposed children in 2005 higher than in 1995.
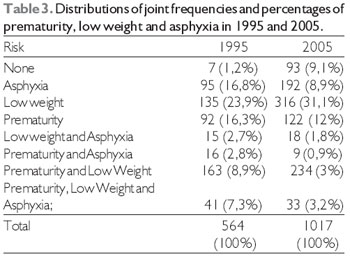
The association between the 3 risk indicators analyzed showed that in the year 1995, 1.2% of the children had none of these, while in 2005 this percentage was of 9.1%. In 1995, the higher percentage noticed between the indicators was of children with Prematurity and Low Weight (28.9%), while in 2005 it was only of Low Weight (31.1%). Still in 1995, there was a simultaneous occurrence of 3 indicators in 7.3% of the children, while in 2005, the percentage was of 3.2%. There was a significant difference between the joint percentage distributions of Prematurity, Low Weight and Asphyxia in both years (p<0.001) (Table 3).
By taking into account the 3 risk indicators and the 3 diseases found, we computed the number of indicators and diseases present in each children. The frequencies and percentages of the numbers found in both years are described in Table 4. In both years the highest number of indicators and diseases noticed in the same children was 3. Most children had a single risk indicator or disease (57.1% in 1995 and 69.4% in 2005). The children born in 1995 tended to have a higher number of risk indicators and/or diseases than those born in 2005 (p<0.001).
From, the review of associations between Prematurity, Low Weight and Asphyxia with Toxoplasmosis, in the years 1995 and 2005; for year 2005, out of 16 suspect cases, 14 (87.5%) did not present any of the risks analyzed and 2 (12.5%) were premature. The only case of Toxoplasmosis confirmed, in 1995, had only Prematurity. The case of Syphilis confirmed in 1995 did not present with any indicator of Prematurity, Low Weight or Asphyxia. In 2005, most cases confirmed or suspected did not present none of such indicators either. Out of 12 cases exposed by HIV, in 1995, 41.7% had Prematurity and 33.3% had no risks of Prematurity, Low Weight or Asphyxia. In 2005 most children exposed (88.3%) had none of the 3 risks.

DISCUSSION
The indicator Prematurity showed a significant difference in the comparison between the years (p<0.001), with a higher prevalence in the newborns of 1995, as well as the indicator Asphyxia that had a higher prevalence in this year (p<0.027), and there was no significant difference only for the indicator Low Weight (p<0.209). Such findings may be justified according to the improvements along the years in the maternity that helped and provided good resources and high qualify professionals to women that seek assistance and follow up during the puerperal period, which decreased the rate of premature newborns and those with Asphyxia along 10 years.
Only Toxoplasmosis, Syphilis and HIV were found and analyzed; this may be explained by the fact that in 1995 the service and attention offered to pregnant women was poor and most tests for identification of diseases transmitted by the mother were not performed. Later on, after the 90's, with the introduction of programs aimed at the woman's health it was possible to draw the attention of a larger group of women from the beginning of the pregnancy to prenatal follow-up, and the triage was more faithful, which alerted the suspicious and confirmed cases of such diseases (19, 20, 21).
When the risk indicators (Prematurity, Low Weight and Asphyxia) and the diseases (Toxoplasmosis, Syphilis and HIV) were analyzed and compared between 1995 and 2005, there was an occurrence of risk indicators higher than of diseases themselves, since the indicators are confirmed right after the birth of these children, which did not rely on more objective and invasive exams for their identification (8, 12, 22).
Upon association of the percentage of cases of Toxoplasmosis in both years (1995 and 2005), with the presence of risk indicators, only the year of 1995 had some relationship, in this case, with Prematurity.
No studies were found that confirmed this finding, but other risk indicators, like Weight at birth, had a better relationship in some studies (23) that found infections as the second most frequent disease in the pregnancy of mothers of Low Weight, and the high number of mothers with Syphilis, Toxoplasmosis and HIV was notorious.
When connected to risk indicators, syphilis did not present any relationship, different from the research results (24) in Guinea-Bissau, which verified a strong association of positive serology for Syphilis with premature birth and natimortality.
When connected to risk indicators, HIV presented cases only in 1995, in which 41% of these related to Prematurity, which confirms some studies (25, 26, 27) that [sic] upon comparison with the occurrence of risk indicators and infecto-contagious diseases for child hearing loss. The most frequent risk indicators were the permanence at neonatal ICU with a longer period than 48 hours and the number of newborns that remained was about 80%. This data was predicted, once most premature newborns need intensive care upon birth.
From the analytic of the data surveyed we could show the importance of the research carried out on risk indicators and the need to improve woman assistance programs for public health and Phonoaudiology. Therefore, the identification of infecto-contagious diseases and risk indicators for deafness from the very beginning of pregnancy and/or the life of a baby may allow the suitable referral to programs of identification and rehabilitation, by decreasing the extension of the sequels on the development of the child. At the same time, with campaigns of adhesion to the programs that promote health, it is possible to decrease such indicators and diseases causing hearing loss.
CONCLUSION
From the data analysis, it was possible to show the occurrence of risk indicators for hearing loss and the importance for public health and Phonoaudiology of the need to improve woman assistance programs. Once the data obtained revealed a higher number of risk indicators in 1995, with improvement along the years, we confirmed programs intended for the woman's health created along 10 years. Therefore, the identification of infecto-contagious diseases and risk indicators for deafness from the very beginning of pregnancy and/or the life of a baby may allow the suitable referral to programs of identification and rehabilitation, by decreasing the extension of the sequels on the development of the child. At the same time, with campaigns of adhesion to the programs that promote health, it is possible to decrease such indicators and diseases causing hearing loss.
BIBLIOGRAPHICAL REFERENCES
1. Andrade GMQ, Resende LM, Goulart EMA, Siqueira AL, Vitor RWA, Januário JN. Deficiência auditiva na toxoplasmose congênita detectada pela triagem neonatal. Rev Bras Otorrinolaringol. 2008, 74(1):21-8.
2. Yoshinago- Itano C, Sedey A, Coulter D, Mehl A. Language development of early and later-identified children with hearing loss. Pediatrics. 1998, 102:1161-1171.
3. Prevots DR, Parise MS, Segatto TC, Siqueira MM, Santos ED, Ganter B et al. Interruption of measles transmission in Brazil, 2000-2001. J Infect Dis. 2003, 187(1):111-20.
4. Pelegrin N. Avaliação e diagnóstico precoce da surdez. In: 1º Encontro Nacional Interdisciplinar na Área da Deficiência Auditiva. Anais. Rio de Janeiro: MEC/INES; 1990, 15-8.
5. Northen JL, Downs MP. Hearing in children. Baltimore: Willims &Wilkins Co; 1991.
6. Joint Committee on Infant Hearing 1994. Disponível em: http://www.jcih.org/history.htm em: 16.08.2008.
7. Nahmias AJ. The TORCH complex. Hosp Prac. 1974, 9:65-72.
8. Pupo AC, Balieiro CR, Figueiredo, RSL. Estudo retrospectivo de crianças e jovens com deficiência auditiva caracterização das etiologias e quadro audiológicos. Rev CEFAC. 2008, 10(1):84-91.
9. Stagno S, Britt W. Cytomegalovirus Infections. In: Remington JS, Klein JO, Wilson CB, Baker CJ. Infectious Diseases of the Fetus and Newborn Infant. 6th ed. Philadelphia: Elsevier Saunders; 2006, 739-81.
10. Silva AA, Maudonnet O, Panhoca R. A deficiência auditiva na infância. Retrospectiva de dez anos. ACTA AWHO. 1995, 14(2):72-5.
11. Kadoya R, Ueda K, Miyazaki C, Hidaya Y, Tokugawa K. Incidence of congenital rubella syndrome and influence of the rubella vaccination program for schoolgirls in Japan, 1981-1989. Am J Epidemiol. 1998, 148(3):263-8.
12. Nóbrega MD, Weckx LLM, Juliano Y. Study of the hearing loss in children and adolescents, comparing the periods of 1990-1994 and 1994-2000. Int J Pediatr Otorhinolaryngol. 2005, 69:829-38.
13. Arvin AM, Whitley RJ, Gutierrez KM. Herpes Simplex Virus Infections. In: Remington JS, Klein JO, Wilson CB, Baker CJ, editors. Infectious Diseases of the Fetus and Newborn Infant. 6th ed. Philadelphia: Elsevier Saunders; 2006.
14. Osis MJD. PAISM: um marco na abordagem da saúde reprodutiva no Brasil. Cad Saúde Pública. 1998, 14 Suppl:25-32.
15. Costa AM. Desenvolvimento e implantação do PAISM no Brasil. In: Giffin K; Costa, SH, organizadores. Questões da saúde reprodutiva. Rio de Janeiro: Fiocruz; 1999, p. 319-35.
16. Victora CG, Barros FC, Tomasi E, Menezes AM, Horta BL, Weiderpass E, César JÁ, Costa JSD, Olinto MT, Halpern R, Garcia MDM, Vaughan JP. Tendências e diferenciais na saúde materno-infantil: delineamento e metodologia das coortes de 1982 e 1993 de mães e crianças de Pelotas, Rio Grande do Sul. Cad Saúde Pública [online]. 1996, 12 (suppl.1):7-14.
17. Serruya SJ, Cecatti JG, Lago TDG. O Programa de Humanização no Pré-natal e Nascimento do Ministério da Saúde no Brasil: resultados iniciais. Cad Saúde Pública. 2004, 20(5):1281-1289.
18. Nagahama EEI, Santiago SM. O cuidado pré-natal em hospital universitário: uma avaliação de processo. Cad Saúde Pública. 2006, 22(1):173-79.
19. Watkin PM. Neonatal otoacustic emission screening and the identification of deafness. Arch Dis Child. 1996, 74(1):16-25.
20. Lichtg I. Audição: abordagens atuais. Pró-Fono. 1997, 4-22.
21. Fowler KB, Dahle AJ, Boppana SB, Pass RF. Newborn hearing screening: will children with hearing loss caused by congenital cytomegalovirus infection be missed? J Pediatr. 1999, 35:60-4.
22. Andrade GMQ, Resende LM, Goulart EMA, Siqueira AL, Vitor RWA, Januário JN. Deficiência auditiva na toxoplasmose congênita detectada pela triagem neonatal. Rev Bras Otorrinolaringol. 2008, 74(1):21-8.
23. Araujo BF, Tanaka ACDA. Fatores de risco associados ao nascimento de recém-nascidos de muito baixo peso em uma população de baixa renda. Cad Saúde Pública [online]. 2007, 23(12):2869-2877.
24. Labbe AC, Mendonça AP, Alves AC, Jaffar S, Dias F, Alvarenga IC, Frost E, Morency P, Milord F, Pepin J. The impact of syphilis, HIV-1 and HIV-2 on pregnancy outcome in Bissau, Guiné-Bissau. Sexually Transmissible Diseases. 2002, 29:157-167.
25. Vieira EP, Miranda EC, Azevedo MF, Garcia MV. Ocorrência dos indicadores de risco para deficiência auditiva infantil no decorrer de quatro anos em um programa de triagem neonatal de um hospital público. Rev Soc Bras Fonoaud. 2007, 12(3):214-20.
26. Abrams EJ, Matheson PB, Thomas PA. Neonatal predictors of infection status and early death among 332 infants at risk of HIV-1 infection monitored prospectively from birth. Pediatrics. 1995, 96:451-58.
27. Goedert JJ, Mendez H, Drumond JE. Mother to infant transmission of human immunodeficiency virus type 1: association with prematurity or low ANTI-gr 120. The Lancet. 1989, 8676:1351-54.
1 Master's Degree in Phonoaudiology by the Pontifical Catholic University of São Paulo (PUC/SP). Preceptor of the Multiprofessional Residence of HU - MA in Phonoaudiology Phonoaudiologist of Neonatal ICU of the Maternity Child HU - Ma.
2 Doctor in Human Communication Disorders (Phonoaudiology) from the Federal University of São Paulo. Clinical director and of research of the Institute of Hearing Advanced Studies Momensohn Santos; Head professor of the Pontifical Catholic University of São Paulo.
Institution: Pontifícia Universidade Católica de São Paulo. São Paulo / SP - Brazil. Mail address: Monique Kelly Duarte Lopes - Rua Tarquinio Lopes, 11A - Anil - São Luís / MA - Brazil - Zip code: 65047-170 - Telephone: (+55 98) 8712-7118 - E-mail: moniqlopes@gmail.com
Article received on August 30, 2010. Approved on November 20, 2010.
|
|
 |
|
|