 |
761 |
|
Year: 2011 Vol. 15 Num. 2 - Abr/Jun - (9º)
DOI: 10.1590/S1809-48722011000200009
|
|
 |
| Section:
Original Article
|
|
|
|
|
| Correlation Between the Audiologic Findings and Tinnitus Disorder |
|
| Author(s): |
| Maria Fernanda Capoani Garcia Mondelli1, Alice Borges da Rocha2.
|
|
|
| Key words: |
| hearing loss, tinnitus, questionnaires. |
|
|
 |
| Abstract: |
Introduction: The correlation between hearing loss with tinnitus can be justified if we consider that this is a tinnitus-causing factor, since the impairments or degenerations on the inner ear and the vestibulocochlear nerve can cause the tinnitus. According to different reports, 85%-96% of patients with tinnitus show some degree of hearing loss. Objective: To correlate the sex, age, degree and type of hearing loss with the tinnitus disorder in patients at the Electronic Devices-related Clinic of Deafness). Method: Retrospective study of exploratory nature in 100 individuals' records duly registered at the Phonoaudiology Clinic of University of São Paulo's Dentistry School in Bauru FOB/USP, by using the THI instrument (Tinnitus Handicap Inventory). Results and Conclusion: Sex, age and degree of hearing loss do not have an influence over the tinnitus disorder, but the hearing loss in tinnitus listeners is progressively bigger according to age and in individual with neurosensorial hearing loss.
|
|
|
INTRODUCTION
Hearing loss is a factor apart from the attack degree affecting the people's quality of life, and when it is acquired in adults, it gradually appears and it makes oral language difficult (1). According to Brazilian Otology Society - SBO (2005) (2), the hearing loss attacks around 70% of the individuals, hence it is a matter of public health with specific requirements regarding health promotion and hearing rehabilitation.
The positive correlation between hearing loss and tinnitus can be justified if we consider that this is the tinnitus-causing factor, since damages or degenerations on the inner ear and the vestibulocochlear nerve can cause tinnitus (3-6). Therefore, it is very reasonable to assume that hearing loss increases the risk that tinnitus can provoke interference with concentration and emotional equilibrium or that it works as a co-factor of this interference, i.e., that the tinnitus disorder is 'contaminated' by the hearing loss disorder (7).
According to different reports, 85%-96% of patients with tinnitus show some degree of hearing loss (8).
Tinnitus is regarded as a sound perception without a presence in the environment (3, 9). It consists of a sensation deemed to be illusory that can be characterized as a noise similar to that of rain, sea, running water, bells, insects, whistles, squeaking, doorbell, pulsation, among others. This sensation can be continual or intermittent and it can show different tone characteristics, be intense or soft, as well as be noticed in the ears or head (10-13).
Epidemiological studies report the tinnitus incidence between 1 and 32% of the population, estimating around 35 to 50 million people in the USA. The incidence is bigger in the elderly population, and it reaches up to 15% in the age group above 65 (14).
Authors refer (15) that tinnitus shows an elevated prevalence, and it is found in 63.3% of the individuals above 45 years of age. Among the losses caused by this symptom, failures in thought, memory and concentration can be found. These alterations can impact leisure activities, relaxation, communication, social and home environment, having an effect on the psychic scope, by provoking irritation, anxiety, depression and insomnia. Approximately 17% of the population is affected by tinnitus, out of which 15% to 25% present an interference with their quality of life (16).
As to the form, it can be continual or intermittent, constant, mono or polytonal. As to intensity, it can vary from an audible tinnitus only in silent rooms to a tinnitus making the individual very uncomfortable. Tinnitus can be considered slight when it is only noticed by the patient in some situations; moderated, when the patient notices its existence but he/she does not feel uncomfortable; intense, when it is unpleasant and causes disorder, jeopardizing daily activities; and severe, when it becomes unbearable, it is unstoppably heard, following the individual all the time.
Some of the several causes of tinnitus, which are hardly isolated, are otologic diseases, cardiovascular alterations, metabolic, neurologic and psychiatric diseases, dental factors and possibly the ingestion of drugs, caffeine, nicotine and alcohol (18).
Researchers (19) have developed a specific questionnaire called Tinnitus Handicap Inventory (THI), which evaluates the emotional, functional and catastrophic features, proving to be easily interpreted and applied. THI is comprised of 25 questions with a score range from 0 to 100, where the bigger the score the bigger is the tinnitus impact in the patient's quality of life. It has been widely used in the clinical context to evaluate patients with tinnitus to quantify the disorder related to this symptom and the evaluation of responses to the proposed treatments.
THI is considered a more comprehensive evaluation method, especially with regard to the psychological and everyday characteristics of tinnitus (20).
According to the research (21) performed with the intention of analyzing the audiologic profile of patients with tinnitus, it has been found, as a result, that the patients served at the clinic frequently complained about tinnitus, and more frequently about the unilateral tinnitus. Neurosensorial hearing loss prevailed, although other types of hearing loss have been detected. Most patients reported to have a constant and unique tinnitus, corroborating with the data found in other studies. The occurrence of tinnitus per age group and gender, and the disease time, is similar to that found in other works relating that tinnitus is more frequent in female, it increases with age, and it is prevalent in older individuals and, in most cases, they are bilateral and unique, and the history time of complaint is longer than 3 years.
Since it is a very common complaint, whose occurrence causes a lot of discomfort to patients, interfering with their professional performance and family relationships, it has been decided to investigate the degree of hearing loss and the tinnitus disorder.
The objective of this work is to correlate the sex, age, degree and type of hearing loss with the tinnitus disorder in patients at the Electronic Devices-related Clinic of Deafness)
METHOD
For this study observing the transverse cut, all the records of patients registered at the Phonoaudiological Clinic of the University of Sao Paulo's Dentistry School in Bauru, FOB/USP have been retrospectively reviewed.
The procedure to analyze and select the patients started after the Ethical and Research Committee has approved it under the number 202/2009.
To compose the sample of this study, some inclusion criteria were established:
a) Age equal to or above 18;
b) Hearing loss of distinct types and degrees with the following characteristics:
- Degree of hearing loss: it was based on the research of pure-tone threshold audiometry at frequencies of 250, 500, 1000, 2000, 3000, 4000, 6000 and 8000 Hz for both right and left ears. The degree of hearing loss was classified by using the audiometric frequency thresholds of 500, 1000, 2000 and 4000 Hz, classified as slight (average from 26 to 40 dBNA), moderate (average from 41 to 60 dBNA), severe (average from 61 to 80 dBNA) and profound (average above 81 dBNA), according to WHO (2007) (22).
- Type of hearing loss: it took into consideration the comparison between thresholds and the airway and osseous pathway of each ear, and it was classified in accordance with SILMAN and SILVERMAN (1997) (23): conductive hearing loss, neurosensorial hearing loss and mixed hearing loss.
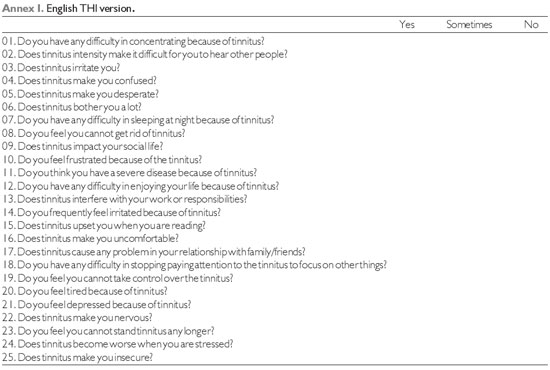
c) Unilateral or bilateral tinnitus and utilization of THI instrument (Annex 1) to quantify the disorder related to this symptom.
THI is comprised of 25 questions, divided into three scales. Functional (F) measures the disorder caused by tinnitus in mental, social, occupational and physical functions. The emotional scale (E) measures the emotional responses such as anxiety, anger and depression. Catastrophic (C) quantifies the desperation and inability to live with or get rid of the symptom, with regard to the attack. There are three options of response for each of the questions, graded as follows: For answers yes (4 points), sometimes (2 points) and no (no point) (19).
Answers were graded from zero, when tinnitus does not interfere with the patient's life, to 100 (points or %), when the disorder degree is severe. The sum of points attained in the questions was categorized into five groups or severity degrees. In accordance with the researchers' proposal (24), tinnitus can be:
degree 1: inconspicuous (0-16%);
degree 2: slight (18-36%);
degree 3: moderate (38-56%);
degree 4: severe (58-76%); or
degree 5: catastrophic (78-100%).
Sex, age, degree and type of hearing loss were correlated with the disorder caused by tinnitus.
For statistical analysis of the data, Spearman's Correlation Coefficient test, Mann-Whitney Test, and Chi Square tests were performed.
RESULTS
1,060 records were analyzed, out of which 100 were selected for this research, in compliance with the inclusion criteria, and 53 of them were female and 47 were male. The age of the evaluated group ranged from 22 to 89, with an average of 62-63 years.
The groups were separated by age group and sex (Graphic 1) for visualization of tinnitus prevalence. It has been observed a gradual increase of tinnitus related to age in both sexes, where females aged 45 or older are prevalent, but this prevalence is not statistically significant (p=0.47), in accordance with Chi-Square Test.
THI degrees achieved are represented in Graphic 2.
In Graphic 3, it has been performed the distribution of THI degrees divided by sex, and a statistically significant correlation (p=0.09) between the sexes has not been found, in accordance with Mann-Whitney test.
The age groups and the tinnitus disorder were correlated, represented by THI results, and it has not been found a statistically significant correlation (p=0.09), in accordance with Spearman Coefficient test, the results are those observed in the Graphic 4.
Graphics 5 and 6 represent the ears evaluated with regard to degree and type of hearing loss.
The degree and type of hearing loss correlated with the tinnitus disorder, it has not been found a statistically significant correlation between both of them, in accordance with Spearman Coefficient, and the results are represented in Graphics 7 and 8.
As to localization of tinnitus, 54 patients mentioned that they felt tinnitus in both ears and 46 believed it was unilateral, and 21 of the latter would mention it was in the right ear and 25 in the left ear, and there was no case where the tinnitus was located in the head.
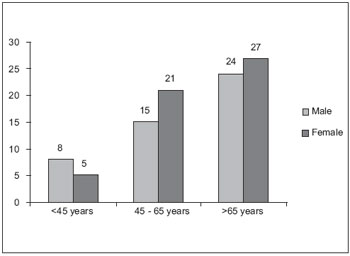 Graphic 1. Correlation between individuals' sex and age.
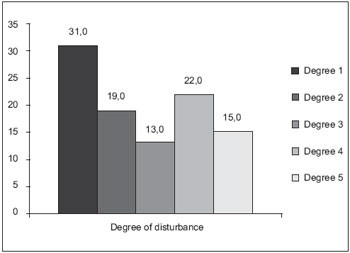 Graphic 2. Degrees of disorder measured by THI questionnaire.
 Graphic 3. Correlation between sex and tinnitus disorder.
DISCUSSION
There was a prevalence of tinnitus in the female sex in most of the age groups, but this prevalence was not significant, and in both female and male sexes, there was a gradual increase of the number of patients complaining about tinnitus as the age increased.
Literature is controversial when observing the tinnitus in both sexes. In our study, there was no difference between male and female, similar to other researchers' findings (25, 26).
Most of the authors who studied the tinnitus incidence in clinics and hospitals found a higher incidence of this complaint in female patients (27, 28) or without a significant difference between the sexes (29-31), corroborating with our findings.
In a previous study (32), where 1,806 patients were analyzed at a Tinnitus Clinic in Portland, Oregon, it has been detected that 69% of patients were male and only 31% were female. This difference is probably because that clinic is a reference to evaluate the legal tinnitus-related features.
We, therefore notice that the studies are paradoxical when relating to the influence of sex in tinnitus prevalence. Some show a discrete augmentation in the prevalence of the female sex, others suggest a higher prevalence of the male sex, but they hardly ever achieve a statistical significance. According to researchers (33), the possible justification for the higher prevalence in the male sex could be related to the fact that men are more exposed to occupational noise, and the biggest prevalence of loss is induced by noise, provoking the tinnitus. However, results (34) have found that women are more careful and concerned about their health, and they search for medical help, what could explain the finding of a higher prevalence in the female sex.
When analyzing the results of THI questioning, measuring the disorder related to patients' sex, we detect that there was no difference caused by the tinnitus in both sexes. These findings corroborate with the data found in another research (35), which also used THI questionnaire, as well as with other authors (36), who used another questionnaire (Tinnitus Severity Questionnaire, TSQ) to evaluate the severity of tinnitus, but they also approached questions of quality of life, difficulties in concentrating, discomfort during silence, depressive reactions, and with researchers' findings (37), who did not notice an influence on sex, age or duration of tinnitus in the disorder caused by the symptom, by using three evaluation questionnaires (Tinnitus Handicap Questionnaire, Tinnitus Reaction Questionnaire, and Subjective Tinnitus Severity Scale).
However, researches (34) concluded that female patients marked significantly higher grades of disorder in the analog-visual scale than male patients. Although different results have been achieved with regard to the influence of the female sex, the evaluation instrument was different, jeopardizing the comparison of results. Nonetheless, it has been found (38) that the female sex is prevalent among patients with severe disorder or sleep alterations, in contrast with our findings.
Average of age found in our study corroborates with literature reports. In a research (26), the results showed a higher prevalence in patients older than 60, in accordance with authors (39), who also observed a higher occurrence in this group, nearly twice as much as the prevalence in the general population, confirming our study. The same occurred with the average with regard to sex, which in accordance with authors (35) there is no statistically significant difference, corroborating with our findings.
Although the highest prevalence of tinnitus with the increase of age, studies show that there is no relation between age and severity of the symptom or the result of the treatment. This finding also corroborates with researchers (37), who did not find an influence of age in the disorder caused by tinnitus, by using THQ, TRQ and STSS questionnaires, and with authors (35), who used THI questionnaire, what corroborates with our findings in this study. However, in accordance with some findings (40, 41), there is a tendency of disorder increase of the tinnitus with age, in contrast with our findings.
Findings of our research are compliant with authors (26), who observed the occurrence of bilateral tinnitus in 56.34% unilateral in 40.00% and in the head in 3.64% of the cases, confirming our findings as well (42), which showed the prevalence of bilateral tinnitus.
We know that tinnitus appears as the result of the dynamic interaction of several centers of the nervous system and the limbic system, and that alterations or cochlea lesions represent only the trigger of the process, causing a disequilibrium in the lower pathways of the hearing system, resulting in abnormal neuronal activity, later intensified by the central nervous system and eventually noticed as a tinnitus (43).
Tinnitus incidence in population with hearing loss is nearly twice as much as that of the population with normal hearing (44). Researches (45) describe that approximately 67% of the patients with hearing loss suffer from tinnitus; half of them say that tinnitus is a problem just as big as or even bigger than their hearing loss.
This way, we can consider that hearing loss is one of the factors causing tinnitus, therefore, hearing loss increases the chances for tinnitus and it can come to interfere with the patient's quality of life.
Researches show that tinnitus severity is related to the degree of hearing loss, and the hearing loss is slight in patients with a low-disturbing tinnitus, and the hearing loss is profound with severely-disturbing tinnitus (40). Authors (37) found a bigger tinnitus impact on the associated hearing loss, for patients without a hearing loss do not seem to be so disturbed.
On the other hand, a research (46) evaluated the relation between THI degrees and the presence or absence of hearing loss in patients with tinnitus. THI data showed that in most cases a subtle or slight degree was correlated with THI for individuals with hearing loss; whilst in patients with tinnitus and normal hearing there was a bigger number of moderate and catastrophic degrees with a statistically significant outcome in comparison with the group with hearing loss. Authors (47) believe that the influence of the hearing loss degree in the severity of the tinnitus is still uncertain, and it finds an irrelevant correlation between hearing thresholds and the tinnitus disorder.
In our study, we observed that the catastrophic degree (degree 5), the biggest tinnitus disorder, was directly correlated with the increase in the hearing loss degree, because it has been noted that, as the hearing loss degree increases, degree 5 was the only one gradually increasing, corroborating with our findings (37,40). This result can be associated with the fact that as a result of the increase in the hearing loss, there is a bigger degeneration of the inner ear, causing a bigger deprivation when hearing environmental sounds and, accordingly, the tinnitus sound becomes prevalent and it comes to disturb this population more intensely.
However, this relation was not observed with all the other degrees, and it was seen no correlation between the hearing loss degree and the degree of tinnitus disorder, confirming other works (46, 47).
In accordance with researchers (43), individuals with sensorial loss typically show a lesion in the external ciliated cells, and this leads to a bigger chance of disproportion and inequality between internal and external ciliated cells, resulting in, in a last analysis, the tinnitus appearance. In a study performed (26), it has been observed that 85% of the patients had audiometry compatible with neurosensorial hearing loss, what corroborates with our work too (34). This data confirms our findings, by showing that the tinnitus associated with neurosensorial hearing loss is prevailing.
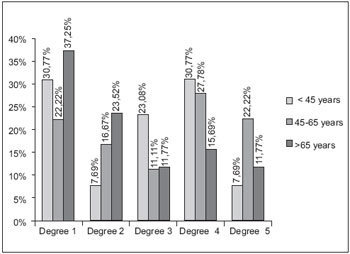 Graphic 4. Correlation between age group and tinnitus disorder.
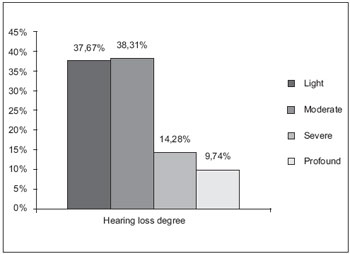 Graphic 5. Average of hearing loss degree in the 154 evaluated ears.
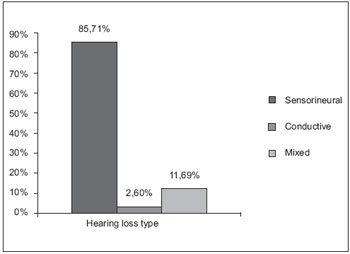 Graphic 6. Average of hearing loss type in the 154 evaluated ears.
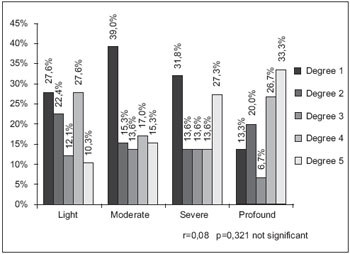 Graphic 7. Correlation between hearing loss degree and tinnitus disorder.
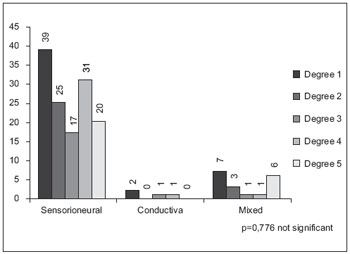 Graphic 8. Correlation between hearing loss type and tinnitus disorder.
CONCLUSION
Sex, age and degree of hearing loss did not have an influence over the tinnitus disorder, but the hearing loss in tinnitus listeners is progressively bigger according to age and in individual with neurosensorial hearing loss.
BIBLIOGRAPHICAL REFERENCES
1. Marchiori LLM, Filho EAR, Matsuo T. Hipertensão como fator associado à perda auditiva. Rev Bras Otorrino. 2006, 72(4):533-40.
2. Sociedade Brasileira de Otologia-SBO. Otologia lança campanha da audição. 2005. Disponível em: www.sbotologia.com.br/09asp. acesso em 02/10/09.
3. Elisabetsky M. Zumbidos: etiopatologia, diagnóstico e tratamento. Folha Méd. 1986, 93(5/6):323-332.
4. Coles RA. Classification of causes, mechanisms of patient disturbance, and associated counseling. In: Vernon JA & Moller AR. Mechanisms of Tinnitus. Boston, Allyn and Bacon. 1995, 11-19.
5. Sanchez TG, Zonato AJ, Bittar RSM, Bento RF. Controvérsias sobre a fisiologia do zumbido. Arq. Fund Otorrinolaringol. 1997, 1(1):2-8.
6. Fukuda Y. Zumbido e suas correlações otoneurológicas. In: GANANÇA, M. Vertigem Tem Cura? São Paulo, Lemos Editorial; 1998, 171-176.
7. Sanchez TG, Medeiros IRT, Levy CPD, Ramalho JRO, Bento RF. Zumbido em pacientes com audiometria normal: caracterização clínica e repercussões Rev Bras Otorrinolaringol. 2005, 71(4):427-31.
8. Sanchez TG, Ferrari GMS. O controle do zumbido por meio de prótese auditiva: sugestões para otimização do uso. Pró-Fono Revista de Atualização Científica. 2002, 14(1):11-8.
9. Jastreboff P J, Sasaki C T. An animal model of tinnitus: a decade of development. Am J Otol. 1994, 15(1):19-26.
10. Ferreira AG, Ferreira N G M, Sierra C M M F. Zumbido: Tratamento cognitivo. Folha Méd. 1986, 93(5/6):123-126.
11. Fukuda Y. Zumbido: diagnóstico e tratamento. RBM-ORL. 1997, 4(2):39-43.
12. Hazell J W P. Models of Tinnitus. In: Vernon JA & Moller A R. Mechanisms of Tinnitus. Boston, Allyn and Bacon; 1995, 57-72.
13. Sanchez, TG. Reabilitação do paciente com zumbido. In: Sociedade Brasileira de Otorrinolaringologia. Tratado de Otorrinolaringologia. São Paulo; Sociedade Brasileira de Otorrinolaringologia; 2002. p.311-24
14. Azevedo AA, Figueiredo RR. Atualização em zumbido. Rev Bras Otorrinolaringol. 2004, 70(1):27-40.
15. Castagno LA, Castagno S. Tinnitus: a clinical study. Folha Méd. 1985, 91(5/6):393-95.
16. Bento RF, Sanches, TG, Minitti A, Câmara J. Zumbido: características e epidemiologia. Rev Bras Otorrinolaringol. 1997, 63(2):229-38.
17. Linden A. Zumbido nos ouvidos. Porto Alegre: ABC da Saúde e Prevenção. Disponível em: http://www.abcdasaude.com.br/artigo.php?481
18. Knobel K, Almeida K. Perfil dos pacientes em terapia para habituação do zumbido (TRT). Fonoaudiologia Brasil. 2001, 1:33-43.
19. Newman CW, Jacobson GP, Spitzer JB. Development of the Tinnitus handicap Inventory. Arch Otolaryngol Head Neck Surg. 1996, 122(2):143-8.
20. Figueiredo RR, Azevedo AA, Oliveira PM. Análise da correlação entre a escala visual-análoga e o Tinnitus Handicap Inventory na avaliação de pacientes com zumbido. Rev Bras Otorrinolaringol. 2009, 75(1):76-79.
21. Miyabara APE, Anastásio ART. Características do zumbido em pacientes atendidos em clínica escola de audiologia. XIV Jornada Fonoaudiológica Prafª Drª Deborah Viviane Ferrari. 2007; 13.
22. WHO - World Health Organization. Grades of Hearing impairment, 2007. Disponível em : http://www.who.int/pbd/desfness/hearing_impairment_grades/en/index.html.
23. Silman S, Silverman CA. Basic audiologic testing. In: Silman S, Silverman CA. Auditory diagnosis: principles and applications. San Diego: Singular Publishing Group; 1997. p. 44-52.
24. McCombe A, Baguley D, Coles R, McKenna L, McKinney C, Windle-Taylor P. Guidelines for the grading of tinnitus severity: the results of a working group commissioned by the British Association of Otolaryngologists, Head and Neck Surgeons, 1999. Clin Otolaryngol Allied Sci. 2001, 26:388-93.
25. Savastano, M. Characteristics of tinnitus: investigation of over 1400 patients. J of Otolaryngol. 2004, 33(4):248-53.
26. Pinto PCL, Hoshino AC, Tomita S. Característica dos pacientes com queixa de zumbido atendidos em ambulatório especializado - HUCFF. Cad. Saúde Colet. 2008, 16(3):437-48.
27. Santos TMM, Branco FCA, Rodrigues PF, Bohlsen YA, Santos NI. Study of the occurence and the characteristics of tinnitus in a Brazilian audiological clinic. In: Proceedings of the Sixth International Seminar, 1999 set 05-09; Cambrige (UK). 543-5.
28. Branco F. Ocorrência e características do zumbido na Irmandade Santa Casa de Misericórdia de São Paulo. São Paulo, 1999. [Monografia - Irmandade Santa Casa de Misericórdia de São Paulo].
29. Fukuda Y, Mota P, Mascardi D. Avaliação clínica de zumbidos: Resultados iniciais. Acta AWHO. 1990, 9(3): 99-104.
30. Martins MC. Zumbido: um estudo de suas características e ocorrência em uma clínica otorrinolaringológica. São Paulo, 1991. [Dissertação - Mestrado - PUC-SP].
31. Sanches L, Boyd C, Davis A. Prevalence and problems od tinnitus in the elderly. In: Proceedings of the Sixth International Seminar, 1999 set 05-09; Cambrige (UK). 1999. 58-63.
32. Meikle MB, Vernon J, Johnson RM. The Perceived Severity of Tinnitus. Some observations Concerning a Large Population of Tinnitus Clinic Patients. Otolaryngol. Head Neck Surg. 1984, 92(6):689-96.
33. Stouffer JL, Tyler RS. Characterization of tinnitus by tinnitus patients. J Speech Hear Dis. 1990, 55(3):439-53.
34. Coelho CCB, Sanchez TG, Bento RF. Características do zumbido em pacientes atendidos em serviço de referência. Arq Int Otorrinolaringol. 2004, 8(3):284-92.
35. Pinto PCL, Sanchez TG, Tomita S. Avaliação da relação entre severidade do zumbido e perda auditiva, sexo e idade do paciente. Bras J Otorhinolaryngol. 2010, 76(1):18-24.
36. Erlandsson SI, Holgers KM. The impact of perceived tinnitus severity on health-related quality of life with aspects of gender. Noise Health. 2001, 3(10):39-51.
37. Méric C, Gartner M, Collet L, Chéry-Croze S. Psychopathological profile of tinnitus sufferers: evidence concerning the relationship between tinnitus features and impact on life. Audiol Neurootol. 1998, 3(4):240-52.
38. Davis AC. Hearing disorders in the population: first phase findings of the MRC national study of hearing. Em: Lutman, ME, Haggard MP, editores. Hearing Science and Hearing Disorders. London: Churchill Livingstone; 1983 p. 35-60.
39. Jastreboff PJ, Gray WC, Gold SL. Neurophysiological approach to tinnitus patients. Am J of Otolaryngol. 1996, 17(2):236-40.
40. Coles RRA. Epidemiology of tinnitus: prevalence. J Laryngol Otol. 1984; Suppl. 9:7-15.
41. Hiller W, Goebel G. Factors influencing tinnitus loudness and annoyance. Arch Otolaryngol Head Neck Surg. 2006, 132(12):1323-9.
42. Sanchez TG, Bento RF, Miniti A, Cârnara J. Zumbido: Características e epidemiologia. Experiência do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo. Rev Bras de Otorrinolaringol, 1997, 63(3):229-35.
43. Jastreboff PJ, Hazell JW. A neurophysiological approach to tinnitus: clinical implications. British J of Audiol. 1993, 27(1):7-17.
44. Coles RRA. Eppidemiology of tinnitus. In: Hezell JWP. (Ed.) Tinnitus.Edinburgh: Churchill Livingstone; 1987, p.46-70.
45. Lindberg P, Scott B, Melin L, Lyttkens L. Long term effects of psychological treatment of tinnitus. Scandin Audiol. 1987, 16:167-72.
46. Savastano M. Tinnitus with and without hearing loss: are its characteristics different. Eur Arch Otorhinolaryngol. 2008, 265(11):1295-300.
47. Baskill JL, Coles RRA. Relationship between tinnitus loudness and severity. In J. Hazell(Ed.), Sixth International Tinnitus Seminar, p. 424-428. Cambridge, United Kingdom: The Tinnitus and Hyperacusis Centre, 1999.
1 Doctor in Communication Disorders from HRAC/USP. Professor Doctor of the Phonoaudiology Department of the School of Basis Dentistry - University of Sao Paulo.
2 Graduated in Phonoaudiology Degree of the School of Dentistry in Bauru - University of Sao Paulo.
Institution: School of Dentistry in Bauru - University of Sao Paulo. Bauru / SP - Brazil. Mailing address: Maria Fernanda Capoani Garcia Mondelli - Alameda Octávio Pinheiro Brizola 9-75 - Vila Universitária - Bauru / SP - Brazil - ZIP Code: 17012-901 - Telephone: (+55 14) 3235-8332 - Email: mfernandamondelli@hotmail.com
CNPq Fomentation
Article received on November 26, 2010. Article approved on February 5, 2011.
|
|
 |
|
|
