 |
863 |
|
Year: 2012 Vol. 16 Num. 2 - Abr/Jun - (19º)
DOI: 10.7162/S1809-48722012000200019
|
|
 |
|
|
| Vestibular system paresis due to emergency endovascular catheterization |
|
| Author(s): |
| Lucinda Simoceli1, Danilo Anunciatto Sguillar2, Henrique Mendes Paiva Santos2, Camilla Caputti2.
|
|
|
| Key words: |
| vestibule of the labyrinth, cardiac catheterization, emergencies. |
|
|
 |
| Abstract: |
Objective: The objective of this story of case is to describe an uncommon cause of associated peripheral Vestibulopathy to the unilateral auditory loss in aged patient after catheterization of urgency. Story of case: Patient of the masculine sort, 82 years, submitted to the correction of abdominal ragged aneurism of aorta, in the intra-operative suffered heart attack acute from the myocardium needing primary angioplasty. High after hospital it relates to complaint of accented hearing loss to the right and crippling vertigo, without focal neurological signals. To the otorhinolaryngological clinical examination it presented: Test of Weber lateralized for the left, spontaneous nystagmus for the left, marches rocking, has taken normal disbasia and ataxia, index-nose and diadochokinesia, Test of Romberg with oscillation without fall and Fukuda with lateral shunting line for the right. The audiometric examination evidenced deafness to the right and sensorineural loss to the left in sharps, areflexia initial to the right in caloric test e, the computerized tomography of the secular bones and brainstem, presence of metallic connecting rod crossing the right secular bone, from the vein internal jugular vein and bulb jugular vein, crossing the posterior, superior and vestibule semicircular canals, projecting itself in temporal lobe. The radiological diagnoses was traumatic injury for guide to endovascular metallic during catheterization of urgency and the behavior, considering that the patient had not compensated the balance, it was vestibular rehabilitation. Conclusion: Complaints of giddiness in the aged patient must be closely evaluated of its pathological clinical description because the antecedents of illnesses and previous treatments, in general, direct the diagnostic hypotheses however they can bring unexpected alterations.
|
|
|
INTRODUCTION
The corporal balance depends on the integration of the vestibular systems, visual and proprioceptive (1,2). Two factors become related with the alterations of balance in the aged one: the gradual increase of the population aging and the proper illnesses of age (2). Amongst them, they are distinguished it vertebral-basilar insufficiency, being able to be represented by ischemic injuries, embolics, desiccants or traumatics (³), alterations of the central nervous system, the metabolic syndrome of disequilibrium of the aged one, hormones alterations/and benign paroxysmal postural vertigo (VPPB) (4). Clinically, the alterations of the balance are characterized for giddiness, vertigo, disequilibrium and fall and are esteem that the prevalence in the aged population arrives the 85% (5,6).
The objective of this story of case is to describe an uncommon cause of associated peripheral vestibulopathy to the unilateral auditory loss in aged patient after catheterism of urgency.
CASE REPORT
Patient of the masculine sort, 82 years, with antecedents of systemic arterial hypertension and dyslipidaemia in medicated treatment, was submitted to the cardiovascular surgery in September of 2000 due the abdominal ragged aneurism of aorta. In the intra-operative it suffered heart attack acute from the myocardium needing primary angioplasty. Since then, it presented history of vertigo to the fast movements of the head and disequilibrium to the changes of decumbency as to seat and to raise and to the deambulation. It remained fifteen days in UTI and it after received high one month hospital from internment with the described complaints and without focal neurological signals. It made use of dihydrocloride of flunarizine per 5 years guided by the cardiologist and kept the complaint of disequilibrium and hyperacusis. To the otorhinolaryngological clinical examination it presented: Test of Weber lateralized for the left, spontaneous nystagmus for the left, marches rocking, has taken normal disbasia and ataxia, index-nose and diadochokinesia, Test of Romberg with oscillation without fall and Fukuda with lateral shunting line for the right.
The audiometric examination evidenced anacusis to the right and sensorineural loss to the left in frequencies 4, 6 and 8 kHz, and the Otolaryngologic Neurological examination evidenced horizontal presence of nystagmus spontaneous for the right with VACL of 3 degrees, oculomotor tests without alterations and vestibular areflexia to the right in the caloric test. It was carried through computed tomography of the secular bones and brainstem, that presence of metallic connecting rod showed crossing the right secular bone, from the vein internal jugular vein and bulb jugular vein, crossing the canals semicircular posterior, superior and vestibule, projecting itself in secular wolf (Figures 1 and 2). The radiological diagnosis was traumatic injury for guide to endovascular metallic during catheterization of urgency and the behavior, considering that the patient had not compensated the balance, it was vestibular rehabilitation. After 40 days of therapy the patient related 90% improvement and after 3 months of therapy, presented complete remission of the disequilibrium symptoms. Actually we found in radiological accompaniment has 3 years without mobilization of the metallic rod.
DISCUSSION
The majority of the authors agrees that, in if treating to alterations of the balance in the aged population, it must be remembered the multifactorial etiology, a time that exist innumerable competing factors of risk, as the presence of neurological illnesses, muscle-skeletal, diabetes, syncope of idiopathic origin, use of different classrooms of drugs, including diuretics, anticonvulsants, antihypertensive, anxyolitics and antidepressant (7,8), cardiovascular illnesses and metabolic riots. These two last ones are main the responsible ones for the attack of the system initial (9,10).
The cardiovascular illnesses are the main causes of mortality in Brazil being that, approximately, 23% of these are represented by heart attack acute of myocardium (IAM) (11). The cardiac catheterism of urgency is one of the therapeutically possibilities in IAM, with rare complicações (12) as for example, vascular injury for the wire guides.
Front to the vertigo complaint, the otolaryngologist doctor must be attempted against to carry through a good clinical history and to investigate causes, of systematic form that justify such symptomatology. In this manner, it is obtained to stipulate reasonable diagnostic hypotheses that can direct, effectively, the treatment. The patient was submitted to the Otolaryngology Neurological clinical evaluation, that included anamneses and otolaryngologist physical examination, audiometry, immittance testing and examination initial, carried through for intermediary of the vectoelectronystagmography, in accordance with the described criteria in literatura (13).
Ahead of findings of anacusis and areflexia initial to right, what it configures a severe cochlea-vestibular that could involve alterations of the internal ear, nerves cochlea-vestibular contests or same brainstem, is essential the request of nuclear magnetic resonance for adjusted diagnóstico (14). One opted to the computed tomography (TC) of secular bones and brainstem since the patient presented phobia when entering in the device of magnetic resonance. The TC was of extreme value therefore closed the injury diagnosis to endovascular catheterism of urgency after. The evaluation for image is used when the clinical inquiry suggests possibility of some responsible central commitment for the symptomatology. The computed tomography is advantageous to bone amendments and the magnetic resonance is optimum method to investigate alterations of soft parts, as for example tumors and degenerações (15).
The patient was submitted the medical evaluations vascular and neurosurgery and guided the radiological control of the picture therefore the withdrawal of the rod could extremely be harmful and it apparently it was presented steady in the bone not generating, at the moment, risks of new endovascular or intra-cranial injuries. Of the otorhinolaryngological point of view, considering that the patient one was aged and presented an unilateral initial areflexia of traumatic origin, with predisposition to the fall, it was opted to therapy of global initial whitewashing (RVG) based in the protocol of CAWTHORNE and COOKSEY associated to the exercises of adaptation of the reflected vestibule-oculomotor. These activities are developed through walked in the street, march with opening and closing of the eyes, object persecution and soccer games (16,17). The procedure was successful in view of that the patient got complete remission of the symptoms to the end of 3 months of treatment. PEDALINI et al. (18) had studied 116 patients amongst which 109 had been analyzed how much to the average time of treatment for attainment of the improvement. The biggest number of patients (n=61) needed 2 months of treatment to relate improvement of the symptoms. POPPER (19) affirms that the RVG is an efficient method, adjusted and innocuous; and that the results gotten in its study had varied since suppression of pathological symptoms, restoration of the balance until the probable "objective cure" of the vestibulopathy.
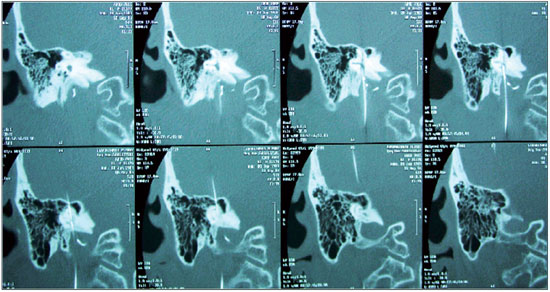 Figure 1. Sequence of images from computed tomography of the temporal bone showing a metal rod (guide wire) injuring the posterior semicircular canals, vestibule and upper, projecting into the temporal lobe.
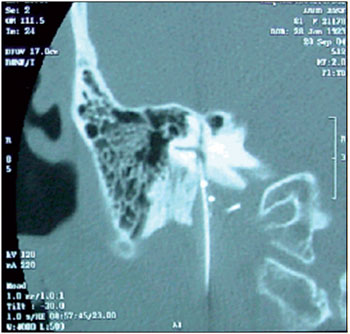 Figure 2. Metal rod through the right temporal bone from the internal jugular vein and the jugular bulb.
FINAL CONSIDERATIONS
Complaints of disequilibrium in the aged patient must be critically evaluated of its pathological clinical description therefore the antecedents of illnesses and previous treatments, in general, direct the diagnostic hypotheses however they can bring unexpected alterations.
BIBLIOGRAPHICAL REFERENCES
1. Matsumura BA, Ambrose AF. Balance in the Elderly. Clin Geriatr Med. 2006, 22:395-412.
2. Konrad HR, et al. Balance and Aging Triological Society Papers: State Of The Art Review. Laryngoscope. 1999, 109(9):1454-1460.
3. Savitz SI, Caplan LR. Vertebrobasilar Disease. Current Concepts. 2005, 352(25):2618-2626.
4. Simoceli L, et al. Perfil diagnóstico do idoso portador de desequilíbrio corporal: resultados preliminares. Rev Bras Otorrinolaring. 2003, 69:772-777.
5. Bittar RSM, Pedalini MEB, Sznifer J, Formigoni LG. Reabilitação Vestibular: Opção Terapêutica na Síndrome do desequilíbrio do idoso. Gerontologia. 2000, 8(1):9-12.
6. Hirvonen TP, Aalto H, Pyykko I, Juhola M, Jantti P. Changes in vestibulo-ocular reflex of elderly people. Acta Otolaryingol Suppl (Stockh). 1997, 529:108-10.
7. Colledge NR, Wilson JA, MacIntyre CC, MacLennan WJ. The prevalence and characteristics of dizziness in an elderly community. Age Ageing. 1994, 23:117-20.
8. Ensrud KE, Nevitt MC, Yunis C, Hulley SB, Grimm RH, Cummings SR. Postural hypotension and postural dizziness in elderly women. Arch Intern Med. 1992, 152:1058-64.
9. Albernaz PLM. Aspectos otoneurológicos na velhice. Acta Awho. 1982, 1(3):93-5.
10. Ganança MM, et al. As tonturas e sintomas associados In: Munhoz MSL, Caovilla HH, Silva MLG. Casos clínicos otoneurológicos típicos e atípicos. São Paulo: Atheneu; 2001, p. 1-22.
11. Secretaria Vigilância em Saúde - Ministério da Saúde - Brasil 2004. www.portal.saude.gov.br/SAUDE/
12. II Diretriz da SBC para tratamento do IAM Arq Bras Cardiol; volume 74, (suplemento II), 2000. www.publicacoes. cardiol.br/consenso/2000/74s2/005.pdf
13. Ganança MM, Caovilla HH, Munhoz MSL, Silva MLG, Frazza MM. As etapas da equilibriometria. In: Ganança MM, Caovilla HH, Munhoz MSL, Silva MLG. Equilibriometria Clínica. Série Otoneurologia. São Paulo: Editora Atheneu; 1999, p. 41-114.
14. Almeida WLC, et al. Vertigem como manifestação isolada de desmielinização no sistema nervoso central: relato de caso e revisão de literatura. Rev Bras Otorrinolaringol. 2004, 70(6):819-822.
15. Menon AD, Sakano E, Weckx LL. Consenso Sobre Vertigem. Rev Bras Otorrinolaringol. 2000, 66(1):9-35.
16. Cooksey FS. Rehabilitation in vestibular injuries. Proc R Soc Med. 1946, 39:273-275.
17. Cawthorne TE. The physiological basis of head exercises. J Chart Soc Physio. Ther. 1944, 29:106-107.
18. Pedalini MEB, Bittar RSM, Formigoni LG, Cruz OLM, Bento RF, Miniti. Reabilitação vestibular como tratamento da tontura: experiência com 116 casos. Arq da Fundação Otorrinolaringologia. 1999, 3(2):74-8.
19. Popper VM. A Reabilitação Vestibular na Vertigem. Centro de Especialização em Fonoaudiologia Clínica, Itajaí, 2001.
1) Doctor in otolaryngology for FMUSP. Responsible for the Sector of Otology of the Hospital Portuguese Charity of São Paulo.
2) Resident of as the year of otolaryngology of the Hospital of the Portuguese Charity of São Paulo.
Institution: Hospital Portuguese Charity of São Paulo. São Paulo/SP - Brazil. Mailing address: Danilo Anunciatto Sguillar - Paes de Barros Avenue, 1425, apartment 122 - São Paulo/SP - Brazil - Zip-code: 03115-001 - Telephone: (+55 11) 3288-0899 - Email: danilo_sguillar@hotmail.com
Article received in March 14, 2010. Article approved in May 16, 2010.
|
|
 |
|
|
