INTRODUCTION Retinoblastoma (RB) is an intraocular tumor affecting especially children (15,000 in 20,000 when born alive) in their first years of life in general. It is of genetic origin affecting the chromosome 13, more specifically the locus 13q14 when in deletion or mutation processes(1).
The effectiveness of chemotherapy for intraocular tumors has been always questionable due to the difficulty for the drugs to pass through ocular limits. Lately, new chemotherapy substances have been tested in order to evaluate their effectiveness on such tumors and the carboplatin has been effectively presenting on the control of the tumor growth(2). Some side effects such as: nephrotoxicity, diarrhea, nausea, vomiting, loss of the hair and ototoxicity(1,2) can be noticed during or after chemotherapy substance administration.
Ototoxic drug usage results in hearing loss, rising toxic reactions of the inner ear by affecting hearing and/or vestibular systems. Aminoglycosides, antineoplasic and loop diuretic agents and others are drugs considered ototoxic type(3,4). Managing drug determines its ototoxic effect, as the use of high quantity only once can damage hearing ability more than if taken in several doses. Besides, hearing ability may vary from patient to patient(5,6).
Spoken language acquisition and development processes are the most important aspects on children's progress, thus it is through language everyone is able to express their feelings, needs and wishes. The hearing sensorial system is directly connected to language development, so the use of diagnostic resources, which brings information on the hearing status of children with RB submitted to chemotherapy the early as possible, has been a routine search by the researchers and professionals, in order to reduce the psychosocial impacts of hearing loss.
The literature has been highlighting two procedures, which has been used in order to early diagnose hearing loss process by ototoxic drugs. They are: audiometry in high frequencies and evoked otoacoustic emissions (EOAEs)(7). Therefore it is important to point that the audiological evaluation in children should follow proper procedures according to age.
It is believed that patients who make use of cisplatin and carboplatin substances undergo lesions in the cochlea, initially on the base in frequencies between 6000 and 8000 Hz (8,9). The impact of hearing loss depends on its degree as well as affected frequencies. Hearing reduction in 6000 and 8000 Hz has low impact on hearing process. Therefore, if such reduction is affected by frequencies above 3000 Hz, there is a higher possibility of damaged speech understanding. If it is lower than 3000 Hz, then, speech understanding is certainly damaged, for being an important area on understanding process(10).
Before all this, the current study aims to verify occurrences of transient evoked otoacoustic emissions (TEOAEs) in patients with RB submitted to chemotherapy with carboplatin substance.
MATERIAL AND METHOD This study was previously approved by the Research Ethics Committee of the INIFESP-EPM, # 0524/04.
Subjects were sent to IOP - GRAAC of UNIFESP - EPM in the audiological clinic department of hearing disorders. The following criteria should be strictly followed by patients for the sample composition:
- Subjects assisted with RB assisted at IOP.
- Subjects with bilateral typanometric curve type A.
- Subjects with no family history of hearing loss.
- Subjects submitted to carboplantin-use chemotherapy.
10 female and 8 male patients aging between nine months and nine years were evaluated after chemotherapy process. The procedure for those patients was from four to six cycles of carboplatin substance (560mg/ m
2/ cycle) with breaks of 21 days.
First proposal suggested by professionals was an audiological evaluation consisted of audiometry and OAE records. Therefore, applying all procedures was not to be meant viable, due to the fact that patients used to come for therapy after the fundoscopic examination, which is performed under sedative use. So, it was performed an exam that did not depend on subject's response and was done in shorter term.
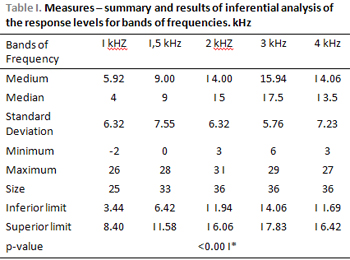
TOAEs RecordsTOAEs records were performed in acoustically designed booth by using ILO 92 - Otodynamics, which was connected to an ACER MATE 486 computer. Patients were laid on parent's lap and then had a probe introduced in their external acoustic canal of each ear. It was presented a nonlinear stimulus click with a range of analysis of 12ms, by using "QuickScreen" program in order to record TOAEs. A load of 260 stimuli was presented in each test, and responses were analyzed in frequencies of 1000, 1500, 2000, 3000 and 4000 Hz.
The exam result considered suitable was: intensity of stimulus ranged between 75 and 80 pe NPS; stimulus stability a 70%; presence of response when general reproductibilty and frequency was a 50% and when sign/noise relation in frequency was a 3 dB NPS on frequencies of 2000, 3000 and 4000 at least.
Statistical Analysis In the current study, the analysis of variance (ANOVA) was considered the most suitable test according to the variables of this study. The level of significance was 0.05 (5%).
RESULTS Charts and tables from measurements and ANOVA will be presented next.
DISCUSSIONData analysis showed 100% of TOAE occurrences on boys and girls. Researches on carboplatin substance did not show expressive hearing loss after its use (11,12,13,14,15). These findings agree with the ones from the current study as all subjects presented with TOAE under the evaluated frequencies. Hearing loss was not expected to occur on current patients because they did not make use of cisplatin substance.
Several researches on ototoxicity of chemotherapic substances were performed with cisplatin, though carbocisplatin was introduced on those researches in the 80s. They observed more use of cisplatin substance due to its toxicity(16, 17, 18, 19, 20, 21, 22, 23, 24).
Hearing loss on frequencies of 4000, 6000 and 8000 Hz was present on patients who made use of carboplatin (25,26). Therefore, involvement of the external ciliated cells with TOAE, which helped the response record up to the frequency of 4000 Hz, was not observed. This finding is related to the procedure used in this study, which is limited, as frequencies of 6000 and 8000 HZ could not be evaluated. Distortion product otoacoustic emissions and audiometry in high frequencies could identify alteration in higher frequencies.
Comparative studies between cisplatin and caboplatin ototoxicity showed hearing loss on frequencies of 4000, 6000 and 8000 Hz in patients who used cisplatin substance as an antineoplasic agent (27,28).
The literature points that cisplatin has greater ototoxic effect than carboplatin. So, the latter do not seem to affect cochlea structures, being considered a less toxic neoplasic agent.
The current study could show that frequencies between 1000 and 4000 Hz were not affected with the use of carboplatin. Longitudinal studies show that individuals presenting hearing loss with frequencies below 3000 Hz are expressively harmed regarding conversations. Children treated with RB by having six cycles of carboplatin (doses of 560mg/m
2) with breaks of 21 days, did not have their social hearing affected (21).
CONCLUSION TOAE occurring in 100% of the cases showed that carboplatin did not cause alteration on external ciliated cells of the cochlea, in the studied frequencies and also TOAE can be used as a tool of evaluation on this population as it is a quick, objective and easy-to-be-tested procedure.
REFERENCES 1. Deegan WF. Novas estratégias para tratamento de retinoblastoma. Ophthalmology Times International, 2004, 8(2):27-31.
2. Kingston JE, Hungerford JL, Madreperla SA. Results of combined chemotherapy and radiotherapy for advanced intraocular retinoblastoma. Arch Ophthalmol, 1996, 114:1321-1328.
3. Skinner R, Pearson ADJ, Amineddine HA, Mathias DB, Craft AW. Ototoxicity of cisplatinum in children and adolescents, 1990, Br J Cancer, 61:927-31.
4. Northern JL, Dows MP. Audição na infância. 5º ed. Rio de Janeiro: Guanabara Koogan; 2005.
5. Laurell G, Jungnelius U. High dose cisplatin treatment: Hearing loss and plasma concentrations. Laryngoscope, 1990, 100:724-34.
6. Brock, PR, Bellman SC, Yeomans EC, Pinkerton CR, Pritchard J. Cisplatin Ototoxicity in children: a practical grading system. Medical and Pediatric Oncology, 19:295-300, 1991.
7. Jacob LCB; Aguiar FP; Tomiasi AA; Tchoeke SN; Bitencourt RF. Monitoramento na ototoxicidade. Revista Brasileira de Otorrinolaringologia, 2006, 72 (6) 836-844.
8. Aguilar-Markulis, Beckley S, Priori R, Mettlin C. Auditory toxicity effects of long-term cis-diamminedicholoroplatinum. Otolaryngol Head Neck Surg, 1981, 89:275-82.
9. Von Der Hults JAM, Dreschler WA, Urbanus NAM. High-frequency audiometry in prospective clinical research of ototoxicity due to platinum derivates. Ann Otol Rhinol Laryngol, 1988, 97:133-7.
10. Meyers FJ, Welborn J, Lewis JP, Flynn N. Infusion carboplatin treatment of rlapsed and refractory acute leukemia: evidence of efficacy with minimal extramedullary toxicity at intermediate doses. Clin Oncol, 1989, 7:173-8.
11. Evans BD, Raju KS, Calvert AH, Harland AH, Wiltshaw E. Phase II study of JM8, a new platinum analog, in advanced ovarian carcinoma. Cancer Treat Rep, 1983, 67:997-1000.
12. Kennedy ICS, Fitzharris BM, Colls BM, Atkinson HC. Carboplatin is ototoxic. Cancer Chemother Pharmacol, 2004, 26:232-4.
13. Bauer FP, Westhofen M, Kehrl W. The ototoxicity of the cystotatic drug carboplatin in patients with head-neck tumors. Laryngorhinootologie, 1992, 71:412-5.
14. Calvert, AH, Harland SJ, Newell DR, Siddk ZH, Jones AC, Mcelwain TJ et al. Early clnical studies with cis-diammine-1, 1-cyclobutane dicarboxylate platinum II. Cancer Chemoter. Pharmacol, 1982, 9:140-7.
15. Castello MA, Clerico A, Deb G, Fidani P, Donfrancesco A. High dose carboplatin in combination with etoposide for childhood tumors. Am J Pediatr Hematol Oncol, 1990, 12:297-300.
16. Kalamark P, Freeman L, Higby DJ, Wallace J, Sinks LF. Clinical response and toxicity cis-Dichlorodiammineplatinum (II) in children. Cancer Treatment Reports, 1977, 61(5):835-39.
17. Helson L., Okonkwo E, Anton L, Cvitkovic E. Cis-platinum ototoxicity. Clin Toxicol, 1978, 13(4):469-478.
18. Paz MI, Codjambossis AD, Pinto UA. Emissiones otoacústicas em la detección precoz de ototoxicidad inducida por cisplatina. Rev Otorrinolaringol Cir Cabeça Cuello, 2000, 60:7-13.
19. Brown RL, Nuss RC, Patterson R, Irey J. Audiometric monitoring os cis-platinum ototoxicity. Gynecologic Oncology, 1983, 16(2):254-62.
20. Von Hoff DD, Schilsky R, Reichert CM, Reddick RL, Rozencweig M, Young RC, Muggia FM. Toxicity effects of cis-dichlorodiammineplatinum (II) in man. Cancer Treatment Reports, 1979, 63(9-10):1527-31.
21. Freilich, RJ, Kraus DH, Budnick AS, Bayer LA, Finlay JL. Hearins loss in children with brain tumors treated cisplatin and carboplatin-based high-dose chemotherapy with autologous bone marrow rescue. Med Pediatr ONCOL, 1996, 71:1039-42.
22. Dishtchekenian A, Iório MCM, Petrilli AS, Azevedo MF. Acompanhamento Audiológico de pacientes com osteossarcoma submetidos a quimioterapia com cisplatina. Revista Brasileira de Otorrinolaringologia, 2000, 66(6):580-90,.
23. Iório MCM, Dishtchekenian A, Garcia AP Petrilli AS. Ototoxicity of cisplatin in osteossarcoma patients. 12 th American Academy of Audiology Annual Convention 2000; Chicago. Annals. Chicago 200. p.146.
24. Domenico ML. Programa de monitoramento auditivo em portadores de osteossarcoma submetidos a tratamento quimioterápico com cisplatina. São Paulo, 2003 (Dissertação de Mestrado - Universidade Federal de São Paulo-Escola Paulista de Medicina).
25. Jacob LCB, Stumpf CC, Bitencourt RF, Marques JM, Puppi C, Gonçalves PT. Avaliação audiológica em indivíduos com neoplasias expostos a agentes quimioterápicos. Fono atual, 2005, 31(8):12-25.
26. Leyraz S, Ohnuma T, Laussus M, Holland JF. Phase 1 study of carboplatin in patients with advanced cancer intermittent intravenous bolus, and 24-hour infusion. J Clin Oncol, 1985, 3:1385-92.
27. Rodriguez-Galindo C, Wilson MW, Haik BG. Treatment of retinoblastoma with vincristine and carboplatin. J Clin Oncol, 2003, 21:2019-2025.
28. Adams M, Kerby IJ, Rocker I, Evans A, Johansen K, Franks CR. A comparison of the toxicity and efficacy of cisplatin and carboplatin in advanced ovarian cancer. Acta Oncol, 1989, 28:57-60.
1. Master degree Speech doctor (expert in Human Communication Disorders by UNIFESP-EPM.
2. PhD in Human Communication Disorders by UNIFESP-EPM. Speech Doctor; Adjunt Professor in the course of Phonoaudiology at UNIFESP-EPM.
3. Speech Doctor - Master degree student in Human Communication Disorders by UNIFESP-EPM.
4. Children Oncologist at Instituto de Oncologia Pediátrica (IOP)* - Grupo de Apoio ao Adolescente e à Criança com Câncer (GRAAC)** - UNIFESP-EPM***.
* Instituto de Oncologia Pediátrica (IOP) - Pediatric Oncology Institute
** Grupo de Apoio ao Adolescente e à Criança com Câncer (GRAAC) - Oncology Children and Adolescent's Supportive Group
*** UNIFESP-EPM - Universidade Federal de São Paulo - Escola Paulista de Medicina (Federal University - Medical School - São Paulo - Brazil)
There was no funding this research.
Aline Mizozoe de Amorim
Address: R Ibituruna 265, ap 71-A, Saúde
CEP: 04051-032, São Paulo/SP
Phone: (11) 5589-1204
This article was submitted to SGP (Publication Management system) of R@IO on May 20th, 2007 and approved on November 6th, 2007 at 12:51:49.